Report on the bacteriological disgnosis and the antitoxic serum treatment of cases admitted to the hospitals of the Metropolitan Asylums Board during the years 1895 and 1896 / by G. Sims Woodhead.
- German Sims Woodhead
- Date:
- [1897?]
Licence: Public Domain Mark
Credit: Report on the bacteriological disgnosis and the antitoxic serum treatment of cases admitted to the hospitals of the Metropolitan Asylums Board during the years 1895 and 1896 / by G. Sims Woodhead. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
38/322 page 14
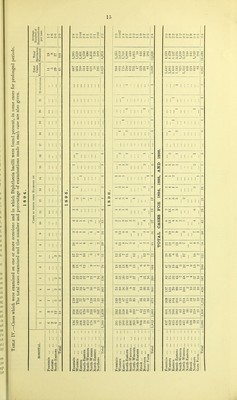
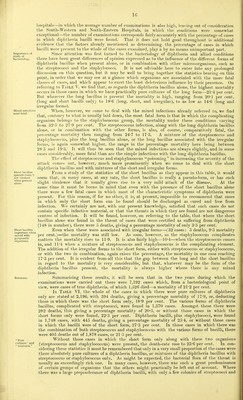
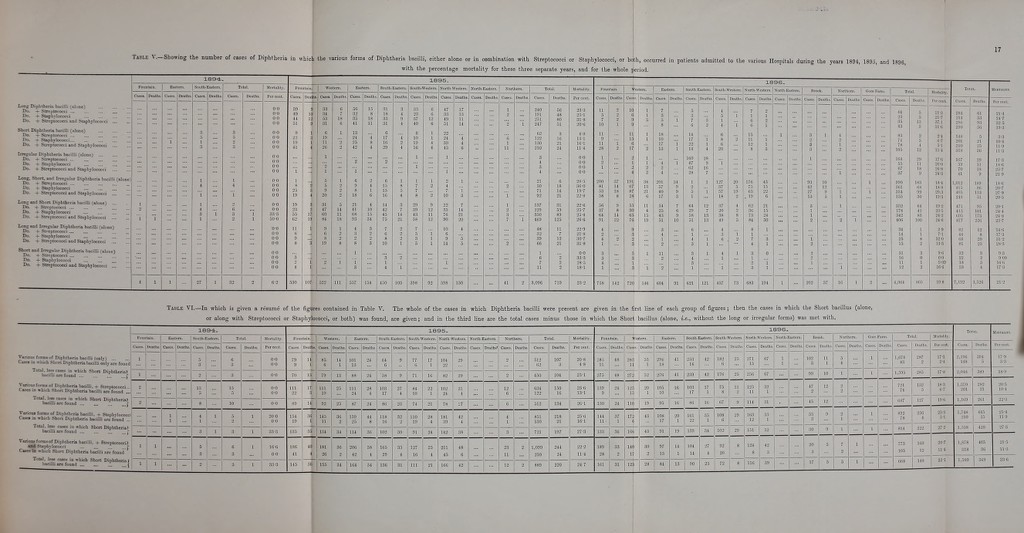
![u Diphtheria bacilli found at last examination. Isolation of patients until bacilli disappear. All doubtful cases to be re-examined Persistence of diphtheria bacilli in throat. On reference to Tables I. and III. it will be noted that out of 12,172 cases, diphtheria bacilli were found at the last examination that was made in no fewer than 4,052, or 33'28 per cent, of the whole. It is interesting to compare the different years in this respect. In 1894, 25 cases out of 45, or 55-5 per cent.; in 1895, 1,594 out of 5,295, or 30-1 per cent. ; in 189G, 2,433 out of 6,832, or 356 per cent., still had diphtheria bacilli in the throat when the last examination was made. Of course it cannot be assumed that all these cases had bacilli in the throat when they were discharged, as at the South-Western Hospital, for example, no second cultivation was, as a rule, sent for examination ; but in a certain proportion of cases there can be no doubt that the patients when discharged had in their throats diphtheria bacilli which, under favourable conditions, might be transmitted from the patient to those with whom he or she afterwards might come in contact. Bearing in mind the continuance of diphtheria in London, and the recognised fact that diphtheria bacilli can be readily transmitted by patients who are apparently no longer suffering from the effects of the disease, to those who have weak or ulcerated throats, I am strongly of the opinion that more attention should be paid to the continued isolation of diphtheria patients in whose throats even slightly virulent diphtheria bacilli still remain. It would, in many cases, necessarily involve detention of the patient in hospital, or isolation over very considerable periods; but it must be remembered that it is just these patients that should remain so isolated or in hospital for a long time that are capable of maintaining in their throats the active agent of infection, and who are, therefore, sources of very great danger to the community, and especially to the children with whom they may come in contact at schools, at home, or during play hours. Another interesting column in this table is that which relates to the cases in which no diphtheria bacilli were -found at the first .examination, although on subsequent examination they were undoubtedly found. In these cases it must be accepted that the clinical diagnosis could not. at first, be in any way corroborated by the bacteriological examination ; but it must also be borne in mind that had no second examination lieen made, and had the cases of diphtheria been of a very mild type, the cases might have been returned as non-diphtheritic in character, so that we have here additional evidence of the necessity for a second examination in all cases in which there is any doubt at all in the mind either of the clinician or of the bacteriologist. In the two following columns we have evidence that under certain conditions the diphtheria bacillus, though undoubtedly present, may, owing to some reason or other (imperfect swabbing out of the throat, the use of antiseptics, or the localisation of the bacilli), be passed over. These cases are considerably fewer in 1896 (92, or 1-34 per cent.) than in 1895 (102, or 1*92 per cent.); so that by increased practice in taking the swabs, improved technique, both in preparation of media and microscopic specimens, and further experience in the examination of the specimens, this source of error may ultimately be reduced to a minimum. There still remains a group of cases which, from the bacteriological point of view, is unsatisfactory, as its presence in the table indicates the possibility of overlooking diphtheria bacilli at the first examination, even when the examination itself appears to be satisfactory. This column is headed : Cases in which no diphtheria bacilli were found at the first examination. As the bacilli were ultimately found, it is evident that in these cases the diphtheria bacillus, though present, was undoubtedly overlooked, except in a very small proportion of cases where infection may have taken place at a period between the two examinations. Leaving 1894 out of account, where the percentage, 8*8, is on a very small number of cases, we find that in 1895 there were 293 cases, or 7-6 ])er cent, of the whole of the cases in which diphtheria bacilli were found, which came under this heading. In 1896 there were 310 cases, or 6'1 per cent.; so that altogether we have a percentage for the three years of 6*7. As these cases were examined on subsequent occasions the error in diagnosis was, of course, ultimately corrected. Here again we have an indication of the importance of making more than a single examination in all cases in which there is any doubt at all, and especially in those cases in which a negative bacteriological diagnosis has, in the first instance, been given. This brings us to the consideration of the cases in which diphtheria bacilli were present over a long period, as evidenced by numerous examinations. In Table IV. is given the number of examinations of the different cases in which diphtheria bacilli were found. In the cases admitted in 1894 none of the specimens were examined more than seven times. In 1895 a few of the specimens were examined much more frequently, three of the cases being examined, one on the 14th, one on the 15th, and one on the 16th occasion respectively, whilst a considerable number were examined from 6 to 13 times, the diphtheria bacillus being found on each occasion. In 1896, when the importance of sending out patients with perfectly clean (as far as the diphtheria bacilli are concerned) throats was evidently becoming more fully recognised, one patient was examined no fewer than 22 times, one 21 times, two 20 times, one 19 times, three 18 times, and a considerable number between 6 and 16 times. It is evident from these figures that some of the cases that were sent out without a second examination may have retained their power of infecting those with whom they might come in contact for very prolonged periods ; it will, indeed, be noted that one or two of the eases remained in hospital for periods of over six months before they were considered to be free from danger from the bacteriological point of view. Although these tables tell their own tale, I may be allowed to draw special attention to the large number of cases in which the diphtheria bacilli persist beyond the first (65-47 per cent.J, second (30-78 per cent.), and third (17-07 per cent.) examinations. The indications for repeated examinations are as marked in this table as they are in the preceding tables. In the last column is given the average number of examinations made in each case. It will be observed that in the Northern and Grore Farm Hospital cases the average number of examinations is very high—3-4 and 3*5 respectively. This average corresponds to the large percentage of notified cases in which diphtheria bacilli were found; whilst in the other](https://iiif.wellcomecollection.org/image/b21518555_0038.jp2/full/800%2C/0/default.jpg)


 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image