Licence: In copyright
Credit: Brain abcess / by Gilbert Horrax. Source: Wellcome Collection.
27/30 page 556
![which had been removed from patients who had been operated upon consecutively by one of my colleagues according to this method [tapping]. He told me of the autopsy findings in a fourth case. He has given up the use of this type of opera¬ tion.” Cairns10 likewise says of tapping : “ We have not found this satisfactory On the other hand, Vincent makes use of repeated taps while waiting for abscesses to encapsulate more thoroughly, but it is intimated that further treatment is usually necessary. Grant, in discussing a paper by Kahn,14 reports the recovery of 5 out of 7 cases from tapping, but this is a mortality of 28 per cent, which is nearly three times greater than the rate given by Macewen, who used open drainage, and more than twice that of our marsupialized cases. Vincent and his associates are the most ardent exponents of complete extir¬ pation of well-encapsulated brain abscesses, and their results have been most striking. Puech, Eliades, and Askenasy15 (1935) reported 8 cases treated by this method, with no deaths from infection, but 2 of the cases died from other causes. My own experience with actual extirpations has been extremely limited, but if it can be accomplished successfully, without drainage, there is no doubt that much time can be saved in hospitalization, for the patient. In the 3 patients of our series drainage was instituted, and, although they all recovered, their course in hospital was as long as the patients treated by marsupialization. CONCLUSIONS 1. The study of a series of 30 brain abscesses covering a period of nine years is presented. 2. The series is divided into two distinct groups, which differ radically from each other both as to their clinical course and classification, their operability, and their prognosis. 3. In the first group—acute and multiple, often metastatic abscesses, usually having severe systemic or pulmonary complications—the outcome is probably always hopeless. 4. In the second group—chronic single, usually encapsulated, abscesses—the prognosis should be favourable, with a mortality not exceeding 10 to 20 per cent, instead of the generally accepted death-rate of 30 to 40 per cent. 5. A discussion of present-day operative methods employed in the treatment of brain abscesses is given, together with certain details of the technique known as £ marsupialization ’, which is here regarded as the treatment of choice. REFERENCES 1 Macewen, Sir William, Pyogenic and Infective Diseases of the Brain and Spinal Cord, 1893. New York : The Macmillan Co. 2 Eagleton, W. P., Brain Abscess : Its Surgical Pathology and Operative Technique, 1922. New York : The Macmillan Co. 3 McKenzie, K. G., “ The Treatment of Abscess of the Brain ”, Arch, of Surg., 1929, xviii, 1594. 1 Grant, F. C., “ The Mortality from Abscess of the Brain ”, Jour. Amer. Med. Assoc., . 1932, xcix, 550. J Cahill, H. P., “ Modern Treatment of Brain Abscess ”, Ibid., 1934, cii, 273. 6 King, J. E. J., “ The Treatment of Brain Abscess by Unroofing and Temporary Hernia¬ tion of Abscess Cavity with the Avoidance of usual Drainage Methods ”, Surg. Gynecol, and Obst., 1924, xxxix, 554.](https://iiif.wellcomecollection.org/image/b30631233_0027.jp2/full/800%2C/0/default.jpg)

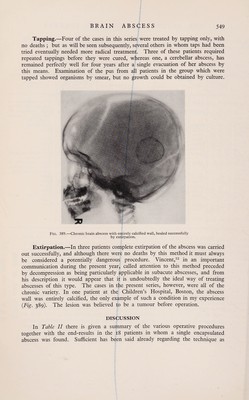



 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image