Volume 1
A manual of medical treatment or clinical therapeutics / by I. Burney Yeo.
- Isaac Burney Yeo
- Date:
- 1894
Licence: Public Domain Mark
Credit: A manual of medical treatment or clinical therapeutics / by I. Burney Yeo. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
57/664 (page 37)
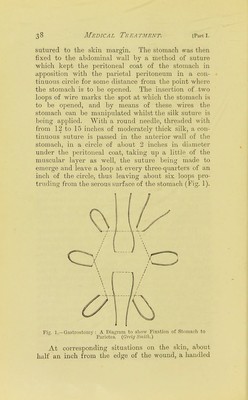
![the skin around the external orifice of the gastric fistula. Dr. Arthur Kempe,* of Exeter, has used this method successfully in a bad case of syphilitic stric- ture situated four inches below the pharynx (which was also deeply ulcerated), in which no food had been swallowed for ten days. In less than three months the patient was able to swallow solid food easily. Professor Annandale has also used retention tubes in treating stricture of the 03so]jhagus, and patients who could swallow fluid with difficulty before, could, after the fixation of the tube in the stricture, swallow easily. He has used them with advantage in both malignant and non-malignant cases. It is only, then, in cases in which the application of txibage seems quite impracticable that the operation of gastrostomy should be resorted to. It should also be always borne in mind, that although when first admitted into the hospital a patient may be quite unable to swallow, yet that after a day or two's rest in bed and the administration of nutrient enemata with opium, the power of swallowing will often be to some extent restored. Mr. Mayo Robson has reported f a case of malig- nant stricture of the oesophagus in which gastrostomy appears to have prolonged life, in a state of compara- tive comfort, for nearly eleven months, during the whole of which time no food was taken excepf. through the artificial opening in the stomach. At the time the operation was performed no food had been taken for several days, and on attempting to pass oesophageal bougies they were always arrested at a point 12| inches from the teeth — not even the sn)allest could be got through the strictui-e. The operation consisted in making a vertical incision 3 inches long at the outer border of the left i-ectus, starting just below the costal margin. The parietal peritoneum was incised to the same extent and * British Medical Journal, Dec. 27, IS'JO, p. 1480. t British Medical Journal, June 7, 1890, p. 12'J5.](https://iiif.wellcomecollection.org/image/b2150930x_0001_0057.jp2/full/800%2C/0/default.jpg)