Licence: Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)
Credit: Infectious multiple drug resistance / S. Falkow. Source: Wellcome Collection.
82/332 page 64
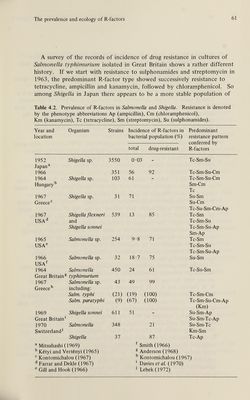
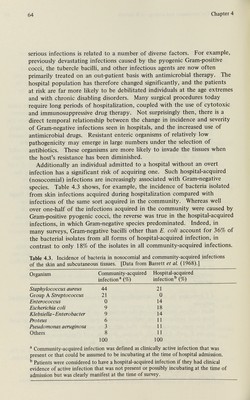
![64 Chapter 4 serious infections is related to a number of diverse factors. For example, previously devastating infections caused by the pyogenic Gram-positive cocci, the tubercle bacilli, and other infectious agents are now often primarily treated on an out-patient basis with antimicrobial therapy. The hospital population has therefore changed significantly, and the patients at risk are far more likely to be debilitated individuals at the age extremes and with chronic disabling disorders. Many surgical procedures today require long periods of hospitalization, coupled with the use of cytotoxic and immunosuppressive drug therapy. Not surprisingly then, there is a direct temporal relationship between the change in incidence and severity of Gram-negative infections seen in hospitals, and the increased use of antimicrobial drugs. Resistant enteric organisms of relatively low pathogenicity may emerge in large numbers under the selection of antibiotics. These organisms are more likely to invade the tissues when the host's resistance has been diminished. Additionally an individual admitted to a hospital without an overt infection has a significant risk of acquiring one. Such hospital-acquired (nosocomial) infections are increasingly associated with Gram-negative species. Table 4.3 shows, for example, the incidence of bacteria isolated from skin infections acquired during hospitalization compared with infections of the same sort acquired in the community. Whereas well over one-half of the infections acquired in the community were caused by Gram-positive pyogenic cocci, the reverse was true in the hospital-acquired infections, in which Gram-negative species predominated. Indeed, in many surveys, Gram-negative bacilli other than E. coli account for 36% of the bacterial isolates from all forms of hospital-acquired infection, in contrast to only 18% of the isolates in all community-acquired infections. Table 4.3. Incidence of bacteria in nosocomial and community-acquired infections of the skin and subcutaneous tissues. [Data from Barrett et al. (1968).] Organism Community-acquired Hospital-acquired infection^ (%) infection'' (%) ® Community-acquired infection was defined as clinically active infection that was present or that could be assumed to be incubating at the time of hospital admission. Patients were considered to have a hospital-acquired infection if they had clinical evidence of active infection that was not present or possibly incubating at the time of admission but was clearly manifest at the time of survey.](https://iiif.wellcomecollection.org/image/b1801964x_0083.JP2/full/800%2C/0/default.jpg)



 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image