Organisation of medical work in the hospital service in Scotland : first report of the Joint Working Party / [Chairman: J.H.F. Brotherston].
- Great Britain. Joint Working Party on the Organisation of Medical Work in the Hospital Service in Scotland.
- Date:
- 1967
Licence: Public Domain Mark
Credit: Organisation of medical work in the hospital service in Scotland : first report of the Joint Working Party / [Chairman: J.H.F. Brotherston]. Source: Wellcome Collection.
33/82 (page 33)
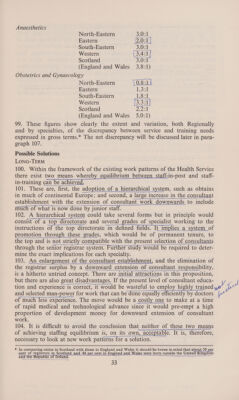
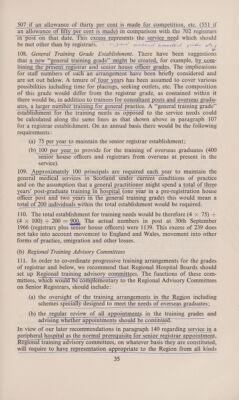
![Anaesthetics North-Eastern 350; | Eastern 2.0:1 | South-Eastern ) SOUF Western \ 3.4 ai Scotland 3.0:1 (England and Wales 3.8:1) Obstetrics and Gynaecology North-Eastern Y0,8:14 Eastern bee South-Eastern Likeak Western [3.3 ef] Scotland Deak (England and Wales 5.0: 1) 99. These figures show clearly the extent and variation, both Regionally and by specialties, of the discrepancy between service and training needs expressed in gross terms.* The net discrepancy will be discussed later in para- graph 107. Possible Solutions LONG-TERM 100. Within the framework of the existing work patterns of the Health Service there exist two means whereby equilibrium between_staff-in-post and staff- in-training can be achiev en a nS Ne AC SEAT 101. These are, first, the adoption of a hierarchical system, such as obtains in much of continental Europe; and second, a large increase in the consultant ee establishment with the extension of consultant work downwards to include er much of what is now done by junior staff. 102. A hierarchical system could take several forms but in principle would consist of a top directorate and several grades of specialist working to the instructions of the top directorate in defined fields. It implies a system_of promotion through these grades, which would be of permanent tenure, to the top and is not strictly compatible with the present selection of consultants sonore aenenancn ta SAMAR SEPE AE Raat FRR AN HES aera ten mrnnesrrminanee ries through the senior registrar system. Further study would be required to deter- mine the exact implications for each specialty. 103. An enlargement of the consultant establishment, and the elimination of the registrar surplus by a downward extension of consultant responsibility, ena gy if ACEC SA NC RATA ATES RAN eaten menmaeeeanian is a hitherto untried concept. There are initial attractions in this proposition, but there are also great disadvantages. If the present level of consultant educa- pasa ts NA SPN es IR science catemennamenaiaetl tion and experience is correct, it would be wasteful to employ highly trained Ee er cecmroon ma TE SI: we! I of much less experience. The move would be a costly one to make at a time of rapid medical and technological advance since it would pre-empt a high proportion of development money for downward extension of consultant work. 104. It is difficult to avoid the conclusion that neither of these two means of achieving staffing equilibrium is, on its own, acceptable. It is, therefore, rena RCATER URC necessary to look at new work patterns for a solution. * In comparing ratios in Scotland with those in England and Wales it should be borne in mind that about 30 per cent of registrars in Scotland and 48 per cent in England and Wales were born outside the United Kingdom and the ‘Republic of Irelan i eis a on](https://iiif.wellcomecollection.org/image/b32184578_0033.jp2/full/800%2C/0/default.jpg)