The throat and nose and their diseases / Lennox Browne ; with special assistance as follows: Anatomy, Mayo Collier ; Nervous diseases, James Cagney ; and Histo-pathology, Wyatt Wingrave.
- Browne, Lennox (Isaac Lennox), 1841-1902.
- Date:
- 1899
Licence: Public Domain Mark
Credit: The throat and nose and their diseases / Lennox Browne ; with special assistance as follows: Anatomy, Mayo Collier ; Nervous diseases, James Cagney ; and Histo-pathology, Wyatt Wingrave. Source: Wellcome Collection.
913/1006 (page 879)
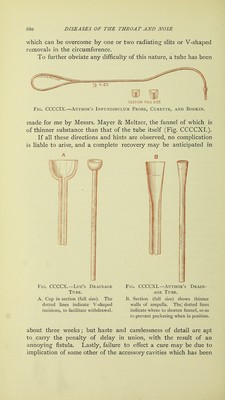
![1. Shave the eyebrow, and cleanse both the external parts and the nasal fossse, the latter by a douche. 2. Make the incision through skin and periosteum carefully along the lower line of the eyebrow—stopping short of the supra-orbital notch. 3. Employ raspatory and retractors for exposing the bone. 4. Employ a trephine sufficiently large to obviate necessity to extend, for the area of this cavity can be thoroughly explored without laying it bare to its whole length. 5. Remove by sharp spoon every particle of the morbid contents before exploring the infundibulum. 6. Pass a suitably curved director by the infundibulum into the nose and out of the corresponding nostril. The direction to be taken is downwards, slightly backwards, and inwards (towards the median line). When in the fossa it must be brought directly forwards. This direction is shown in the illustration (Fig. CCCCVI.). 7. The infundibulum may now require to be enlarged and to be curetted, a difficult procedure by any instrument at present in use. I have therefore constructed a director (Fig. CCCCIX,), which, when once passed, can have fixed to its end a curette, and when this has served its purpose, the next step is— 8. That of threading and withdrawing back to the upper wound : this can be effected with the same instrument. 9. Attach to the thread a Luc or author's drainage tube (Figs. CCCCX. and CCCCXI.), and draw it back through the nostril, so that the cup rests on the floor of the sinus. 10. The cavity having been cleansed and swabbed with a zinc chloride solution about 5 to 6 per cent., the external wound is to be entirely closed, by being brought together with gut sutures. 11. [Some surgeons are careful to insert deep sutures through the periosteum, in addition to the superficial through the skin, but this procedure is not recommended, as it only retards union.] 12. The after-treatment is simple : the drainage tube, which, while in situ, is irrigated twice or thrice daily, is later to be removed by drawing it outwards through the nostril. If, as is probable, there is no surgical fever, no haste should be displayed in taking this tube out; and pain unaccompanied by increase of temperature is no indication for its removal. The longer the tube is left, the more complete will be the drainage, the more permanent the patency of the enlarged infundibulum, and the closer and firmer the union of the wound of incision. The tube should never be withdrawn earlier than the fifth day, and may with advantage be retained till the eighth or tenth. It is of course important to see that it is not blocked, and to continue irrigation even if there be no discharge. Some difficulty may be experienced in removal of the tube : this will be due to two causes, firsts the liability to forget that the axis of the infundibulum is not that of the nares. The tube is therefore to be drawn not directly downwards, but, being grasped in a pair of long-bladed strong forceps, passed up as close to the hiatus as possible, a forward direction should be given, so as to make exit from the nostrils at almost a right angle. The second difficulty is caused by an unnecessarily large cup to the ampulla of the tube, but in any case this is an obstacle](https://iiif.wellcomecollection.org/image/b20410050_0913.jp2/full/800%2C/0/default.jpg)