Volume 2
Reports of the Sleeping Sickness Commission of the Royal Society.
- Royal Society (Great Britain). Sleeping Sickness Commission
- Date:
- 1903-19
Licence: Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)
Credit: Reports of the Sleeping Sickness Commission of the Royal Society. Source: Wellcome Collection.
Provider: This material has been provided by Royal College of Physicians, London. The original may be consulted at Royal College of Physicians, London.
31/84 page 19
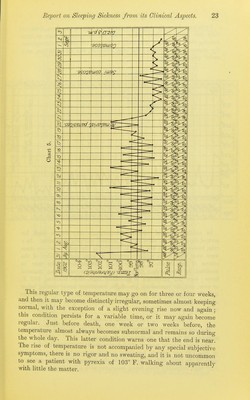
![course, progressing however to its ultimate fatal termination. It is about this time that one usually sees the case, and an ordinary inspec- tion will reveal many of the following points :—There is the dull, heavy, stupid look, a slowness in answering questions, and when speech does come it is often mumbling, slow and thick; the gait is best expressed by the term shuffling. Headaches, vague pains and chest pains may be complained of. The tongue may or may not at this time show the characteristic fine tremor, and in some cases this may also be noticeable in the hands. The skin is often soft and smooth, or it may be slightly roughened. Glandular enlargements common amongst all natives may be prominent, but in some cases this may be very slight. The temperature—a very important point— is elevated, rising in the evenings to 101° or 102° F., falling to subnormal in the morning, the range often extending over 4° or more, and the prJiSe of very low tension is accelerated, varying from 90—130 beats per minute. These two symptoms are of the greatest diagnostic importance in the early recognition of the disease. On interrupting the examination and quietly watching the patient, he will probably sit down, his head may nod, his eyes close, and he remains in this drowsy lethargic condition until again asked some question. If one take such a case into hospital, for the first few days a slight improve- ment may take place; the patient gets up from his bed daily, sits about the doors of the hospital, sometimes walks about outside and takes a little more interest in life, especially at meal times. Soon, however, depending on whether the disease is to run an acute or chronic course, the individual gets worse, he stays in bed more, becomes more drowsy and lethargic, though not actually sleeping, walking at the same time becomes more difficult, and he eventually remains constantly in bed. Tremors now usually become marked, these being of a fine nature. They are best seen in the tongue and arms. The skin may become rough and lose its lustre, but eruptions, though they have been described, are not common. Emaciation and general weakness becomes pronounced; the knee reflexes, which were at first somewhat ex- aggerated, become diminished, the motions are passed involuntarily in bed, and saliva often dribbles from the mouth. Drowsiness, which has gradually been increasing, now passes on to coma, from which the patients can only be roused with difficulty; the temperature falls to subnormal, in rare cases convulsive fits appear, and the patient dies in a complete state of coma. This is the common course of an ordinary acute case of the disease, the different changes taking about a month or six weeks for completion. In the chronic cases the symptoms develop more slowly, and they remain more constant for considerable periods of time without any advance, but ultimately the patients pass into the later stages descri])ed above and eventually die. J) 2](https://iiif.wellcomecollection.org/image/b24750530_0002_0031.jp2/full/800%2C/0/default.jpg)