The student's guide to the diseases of women / by Alfred Lewis Galabin.
- Galabin, Alfred Lewis, 1843-1913.
- Date:
- 1881
Licence: Public Domain Mark
Credit: The student's guide to the diseases of women / by Alfred Lewis Galabin. Source: Wellcome Collection.
124/434 (page 106)
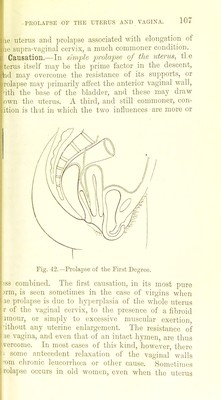
![DISEASES OF WOMEN. near the upper extremity of a Hodge's pessary. Tb former of these is, perhaps, the most likely of any tt prove useful if a stem pessary is tried for the relief! anteflexion « the latter keeps the uterus more effectual in position in retroflexion. PROLAPSE OP THE UTERUS AND VAGINA. Pathological Anatomy.—From the close connection of the uterus with the bladder and anterior vagina], wall, these structures necessarily take part in all dowm ward displacements, and it will therefore be convenient!! to consider prolapse of the vagina in association with prolapse of the uterus. Descent of the uterus has* commonly been termed prolapsus so long as the cervix;] remains within the vulva, and procidentia when it passes outside, although, from the derivation of the words, an opposite usage would have been more appro-« priate. A better classification is that of Dr. Thomas ii into three stages of prolapsus—the first stage, in which the uterus remains entirely within the vulva (Fig. 42); the second, in which it passes partially outside (Fig. 43): and the third, in which the Avhole uterus is extruded J externally (Fig. 44). As the uterus descends, the cervix tends to move in the direction of the vagina as being that of least resistance, and thus the axis of the uterus follows the curved axis of the pelvis, and becomes ■ more and more retroverted in proportion as it becomes lower (Fig. 42). The two chief causes of retroflexion i then come into play (see p. 69), so that this displace- ment is commonly added to retroversion, and the fundus lies low in the hollow of the sacrum (Figs. 26 and 43). When the uterus is finally extruded, it is always in a position of combined retroversion and retroflexion (Fig. 44), unless it has been previously fixed in a position of anteflexion by the presence of a fibroid tumour or other such cause. An important distinction must be made between simple prolapse ot](https://iiif.wellcomecollection.org/image/b2042050x_0126.jp2/full/800%2C/0/default.jpg)