Difficult labour : a guide to its management for students and practitioners / by G. Ernest Herman.
- Herman G. Ernest (George Ernest), 1849-1914.
- Date:
- 1901
Licence: In copyright
Credit: Difficult labour : a guide to its management for students and practitioners / by G. Ernest Herman. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
33/488
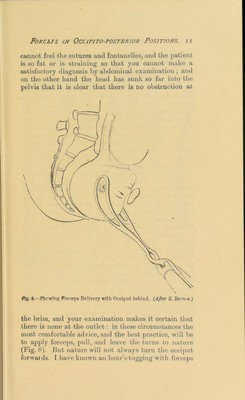
![Treatment in First Stage. Then we get difficulty. If the child is not unusually small, or the uterus unusually strong, help will he needed. If the forehead remains in front, so that it becomes fixed behind the pubic arcli, wffiile the occiput passes over the perineum, the occipito-frontal diameter of the child has to }>ass the antero-posterior diameter of the [iclvic outlet. Now as this diameter measures on an average four inches and a luilf, while the antero- posterior diameter of the outlet varies between four inches and four inches and a half, it will be clear that the head cannot pa.ss easily, and perhaps may not be able to pass at all until it has been a good deal moulded. The perineum is stretched more than it should be, for the diameter which should distend the perineum, the sub-occipito-frontal, only measures four inches, while here the })erineum is stretched by the four inches and a half of the occipito-frontal diameter. Hence a bad rupture of the perineum is more likely to happen when the head is delivered in this position. Treatment.—How is this difficulty best avoided or overcome 'I 1. Preventive: Before rupture of membranes. —The diagnosis of 4in occipito-posterior position ought to be made'^early, by abdominal palpation. Unless the patient be fat, or the abdominal walls rigid, it will be easy for you, if you have practised abdominal palpation as you ought to practise it, to find out that the abdomen is in front before the membranes have ruptured, and, if you have been called in time, before the dilatation of the os has begun. If, then, you are called to a case in which, on palpating the abdomen, in place of the broad, smooth convexity of the back, you feel the little movable knobs which the foetal limbs feel like, at once turn the back forwards. Before the membianes have ruj)tured, this is easily done. Suj)])ose that the child’s belly looks forwards and to the left. Its anterior shoulder will be to the right and in front. -Standing by the side of the patient, put your hands on the abdomen, the right hand behind the child’s anterior shoulder, the left hand in](https://iiif.wellcomecollection.org/image/b21719950_0033.jp2/full/800%2C/0/default.jpg)