A manual of operative surgery / By Lewis A. Stimson ... and John Rogers, jr.
- Lewis Atterbury Stimson
- Date:
- 1895
Licence: Public Domain Mark
Credit: A manual of operative surgery / By Lewis A. Stimson ... and John Rogers, jr. Source: Wellcome Collection.
Provider: This material has been provided by the Augustus C. Long Health Sciences Library at Columbia University and Columbia University Libraries/Information Services, through the Medical Heritage Library. The original may be consulted at the the Augustus C. Long Health Sciences Library at Columbia University and Columbia University.
82/628 page 76
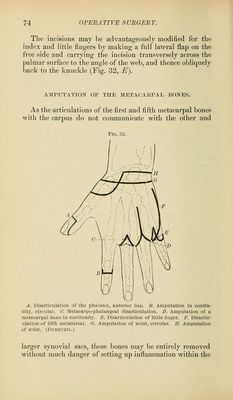
![radius, and the disarticulation completed while the hand is drawn firmly away from the arm. Antero-posterior Flaps. The absence of muscular fibres at the wrist deprives this method of most of the advantages which it offers at other points, and the projection on the palmar surface of the trapezium and pisiform bones renders its execution difficult, and makes it practically identical with the circular method supplemented by lateral incisions. It should be reserved for cases in which the skin is so infil- trated that it cannot be readily dissected back. An incision curved downward is carried across the back of the wrist from one styloid process to the other, the flap dissected up, the hand flexed forcibly, the extensor tendons divided, the joint opened beneath them, and the palmar flap, which should extend as far down as the base of the meta- carpal boues, cut from within outward. Or the palmar flap may be made from without inward, or by transfixion, before the joint has been opened. External Lateral Flap. Dubrueil1 (Fig. 32, H). The hand is pronated, and the operator makes a curved incision, which, beginning on the dorsal aspect a quarter of an inch below the radio-carpal articular line, at the junction of the outer and middle thirds, passes downward, crosses the outer side of the first metacarpal bone at its centre, and returns to a point on the palmar surface opposite that at which it began. Its two ends are then joined by a transverse inci- sion passing around the inner side below the end of the ulna. The external flap is dissected up, the joint opened at the radial side, and the disarticulation completed. AMPUTATION OF THE FOKEARM. The forearm may be divided, with reference to surgical considerations, into upper, middle, and lower thirds. Its shape is cylindrical near the elbow, and gradually flattens and narrows toward the wrist. The lower half of the radius 1 Mcdeeine Operatoire, ]>. 171.](https://iiif.wellcomecollection.org/image/b21206521_0082.jp2/full/800%2C/0/default.jpg)

 No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image No text description is available for this image
No text description is available for this image