Licence: Public Domain Mark
Credit: Remarks on the heart in debility / by G. A. Gibson. Source: Wellcome Collection.
Provider: This material has been provided by the Royal College of Physicians of Edinburgh. The original may be consulted at the Royal College of Physicians of Edinburgh.
10/14 (page 36)
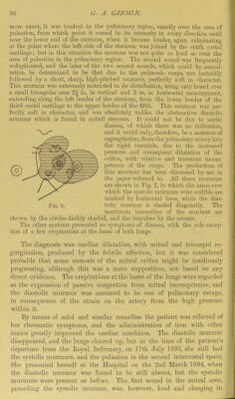
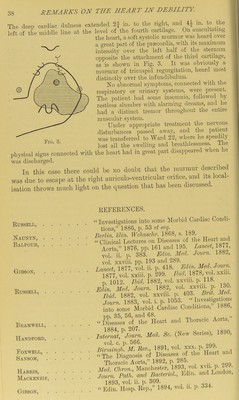
![more exact, it was loudest in the pulmonary region, exactly over the area of pulsation, from which point it waned in its intensity in every direction until near the lower end of the sternum, when it became louder, again culminating at the point where the left side of the sternum was joined by the sixth costal cartilage; but in this situation the murmur was not quite so loud as over the area of pulsation in the pulmonary region. The second sound was frequently reduplicated, and the later of the two secoird sounds, which could by auscul- tation be determined to be that due to the pulmonic cusps, was instantly followed by a short, sharp, high-pitched murmur, perfectly soft in character. This murmur was extremely restricted in its distribution, being only heard over a small triangular area 2\ in. in vertical and 2 in. in horizontal measurement, extending along the left border of the sternum, from the lower border of the third costal cartilage to the upper border of the fifth. This murmur was per- fectly soft in character, and was absolutely unlike the obstructive diastolic murmur which is found in mitral stenosis. It could not be due to aortic disease, of Avhich there was no indication, and it could only, therefore, be a murmur of regurgitation, from the pulmonary artery into the right ventricle, due to the increased ])ressure and consequent dilatation of the orifice, with relative and transient incom- petence of the cusps. The production of ^ this murmur has been discussed by me in ^ the paper referred to. All these murmurs are shown in Fig. 2, in Avhich the areas over Avhich the systolic murmurs were audible are marked l)y horizontal lines, while the dias- Fig. 2. tolic murmur is shaded diagonally. The maximum intensities of the murmur are shown by the circles darkly shaded, and the impulses by the crosses. The other systems presented no .symptoms of disease, Avith the .sole excep- tion of a feAv crepitations at the bases of both lungs. The diagnosis Avas cardiac dilatation, with mitral and tricuspid re- gurgitation, produced by the febrile affection, but it was considered probable that some stenosis of the mitral orifice might be insidiously progressing, although this was a mere supposition, not based on any direct evidence. The crepitations at the bases of the lungs were regarded as the expression of passive congestion from mitral incompetence, and the diastolic mui’mur was assumed to be one of pulmonary escape, in consequence of the strain on the artery from the high pressure within it. By means of salol and similar remedies the patient was relieved of her rheumatic symptoms, and the administration of ii’on with other tonics greatly improved the cardiac condition. The diastolic murmur disappeared, and the lungs cleared up, but at the time of the patient’s departure from the Eoyal Infirmary, on 17th July 1893, she still had | the systolic murmurs, and the pulsation in the second intercostal space. She presented herself at the Hospital on the 2nd March 1894, Avhen the diastolic murmur was found to be still absent, but the systolic murmurs were present as before. The first sound in the mitral area, preceding the systolic murmur, was, however, loud and clanging in](https://iiif.wellcomecollection.org/image/b21969826_0010.jp2/full/800%2C/0/default.jpg)