A clinical text-book of medical diagnosis for physicians and students based on the most recent methods of examination / by Oswald Vierordt.
- Oswald Vierordt
- Date:
- 1900
Licence: Public Domain Mark
Credit: A clinical text-book of medical diagnosis for physicians and students based on the most recent methods of examination / by Oswald Vierordt. Source: Wellcome Collection.
Provider: This material has been provided by the Francis A. Countway Library of Medicine, through the Medical Heritage Library. The original may be consulted at the Francis A. Countway Library of Medicine, Harvard Medical School.
65/642 (page 59)
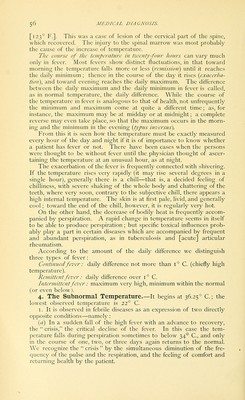
![temperature may give notice of collapse, or a change to a fatal issue, or an internal hemorrhage, as of the bowels in typhoid fever. In the following the most important typical courses of fever are briefly set forth : I. Continued fever exists especially in two diseases, typhoid fever and croupous pneumonia; also in typhus fever, sometimes in erysipelas Day of disease: T. 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 R. P. inillllllBBBBBISSSSSS^IIinil sBsaiBSissaisiissBillnii:^ ■MKiMBaaaaaiiMBiMHB 80 180 170 70 160 150 60 140 130 50 120 110 40 100 90 30 80 70 20 60 41.0 40.5 40.0 39.5 39.0 38.5 38.0 37.5 37.0 36.5 36.0 35.5 35.0 Fig. 4.—Typhoid fever, slight, with tolerably severe recurrence of fever. Maiden, 10 years of age. and miliary tuberculosis. In a case of severe fever, with the diagnosis doubtful, a fever continued through several days points with proba- bility to typhoid fever, and next to acute miliary tuberculosis. In abdominal typhus [typhoid fever] the fever rises for several days by equal steps— initial period; reaches the summit, at which it remains as a continued fever one, two, or more weeks; then, as a Day of disease: 3 4 5 6 7 70 40 30 20 Fig. 5.—Fatal uncomplicated typhoid fever. Temperature and pulse cross each other. Female, age 37. rule, it gradually becomes a remittent fever of such a character that at first the daily maximum remains high, with the minimum going lower (the double stage [the long-continued paroxysm]—the mini- mum may even go below the normal); then the defervescence begins, the maximum declining; this usually reaches the normal in a few days. The remittent and defervescent stages may be protracted for](https://iiif.wellcomecollection.org/image/b21082364_0065.jp2/full/800%2C/0/default.jpg)