Volume 1
A text-book of medicine for students and practitioners / by Adolf v. Strümpell.
- Adolph Strümpell
- Date:
- 1911
Licence: Public Domain Mark
Credit: A text-book of medicine for students and practitioners / by Adolf v. Strümpell. Source: Wellcome Collection.
67/874 page 39
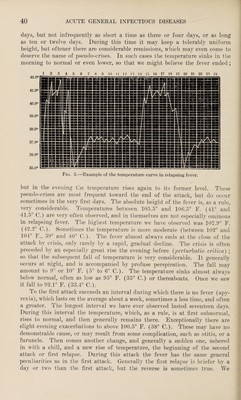
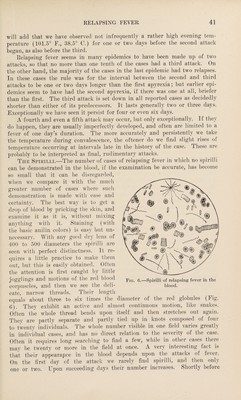
![lation with the blood of patients. This has been established by a Russian physician, by the experimental inoculation of healthy persons. Doctors have been repeatedly inoculated at the autopsy of those who have died of relapsing fever. The disease may likewise be transferred by inoculation to monkeys, while other mammals seem to enjoy an immunity from it. [The first cases of relapsing fever observed in this country were in Irish immigrants coming over in the same vessel in the year 1844. At several peri¬ ods since then more or less limited outbreaks traceable to immigration have occurred, but the disease has never acquired any foothold with us, and com¬ paratively few physicians have ever seen it. So far as can be learned, only one case has ever been seen in Boston, and that was in the person of a physi¬ cian from another city, who brought the disease with him and passed through it in the Massachusetts General Hospital.] Clinical History.—The stage of incubation lasts about five to eight days. It is only exceptionally that some slight prodromal symptoms present them¬ selves just before the outbreak of the disease proper. As a rule, it begins sud¬ denly, with a more or less pronounced chill and intense constitutional symp¬ toms. There are violent headache, great languor, anorexia, and especially marked pains in the loins and extremities. The temperature rises rapidly, reaching generally 106° F. (41° C.) or higher as early as the first or second day. The skin is hot and dry, and usually quickly assumes a very characteristic dirty-yellowish color. In Leipsic we often saw herpes labialis, which seems, however, to have been rarer in epidemics elsewhere. The tongue becomes dry and thickly coated. Sometimes there is vomiting. The bowels are consti¬ pated, or there is a slight diarrhea. The spleen becomes rapidly enlarged, being, as a rule, even larger than in typhoid or typhus. The liver is slightly enlarged. The chest presents the signs of a bronchitis, generally moderate, but in exceptional instances severe. The pulse is much quickened. It is sel¬ dom that there are severe cerebral symptoms beyond a certain apathy and stupor. We have seen delirium tremens, sometimes, in drunkards. A very characteristic symptom, already mentioned, is the marked hyperesthesia of the muscles, especially in the calves. After these symptoms, accompanied by persistent and generally very high fever, have lasted five days to a week, there is a critical decline of tempeiatuie, with'profuse sweating. The patient now improves so rapidly and decidedly that he thinks himself completely cured, and generally gives little credence to the physician’s prophecy of a relapse. In rare but wTell-attested cases there has been really but one attack. The rule is that, after about a week, a second attack occurs, often a third after that, and, infrequently, even a fourth and fifth. In each of these, the above-mentioned symptoms are repeated more or less completely and violently. As the only certain and constant sign of the recurring attacks (the so-called relapses) is a fresh rise of temperature, it will be well to consider their peculiarities at the same time that w^e describe the course of the fever. During the intervals of normal temperature the other objective symptoms of disease are usually absent, except an evident splenic tumor, and, not infrequently, the peculiar pale-yellow hue. Course of the Fever (see Fig. 5).—The beginning of the fever in the first attack is, as we have said, almost always sudden, so that it may even in a few hours reach a considerable height. The fever lasts, as a rule, five to seven](https://iiif.wellcomecollection.org/image/b3136276x_0001_0067.jp2/full/800%2C/0/default.jpg)