The cyclopaedia of practical medicine: comprising treatises on the nature and treatment of diseases, materia medica and therapeutics, medical jurisprudence, etc., etc (Volume 2).
- Date:
- 1845
Licence: Public Domain Mark
Credit: The cyclopaedia of practical medicine: comprising treatises on the nature and treatment of diseases, materia medica and therapeutics, medical jurisprudence, etc., etc (Volume 2). Source: Wellcome Collection.
Provider: This material has been provided by the National Library of Medicine (U.S.), through the Medical Heritage Library. The original may be consulted at the National Library of Medicine (U.S.)
17/808
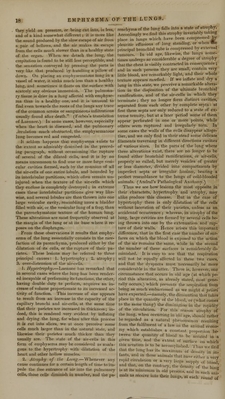
![find a more appropriate place in the articles re- spectively allotted to these subjects. Emphysema of the lungs alone forms an exception, and will therefore be treated of in the next article. R. TOWNSEND. EMPHYSEMA OF THE LUNGS.— The morbid appearances presented by this disease have been noticed by Bonetus, Morgagni, Van Swreten, Storck, and other anatomists. In this country we have a verv correct account of an emphysematous lung from the pen of Sir John Floyer; and Dr. Baillie's work on Morbid Anatomy contains an accurate description of the three principal circum- stances which characterize this lesion, namely, the great size of the lungs, the dilatation of the cells, and the vesicles formed by extravasation of air under the pleura. The discovery of its fre- quent occurrence as a disease, of its etiology, and diagnosis, was, however, reserved for the patholo- gical researches of M. Laennec. [An excellent assay on the subject has been published by M. Louis (translated by Dr. T. Stewardson of Phi- ladelphia) in Dunglison's Medicttl Library for 1838.] In order to render the following observa- tions intelligible, it will be necessary to premise a few observations on the anatomical structure of the pulmonary parenchyma, as the emphysematous condition of tins viscus is, in many cases, merely an exaggeration of its natural or healthy struc- ture. If we examine in a good light the surface of a sound lung, we can ascertain by the naked eye, through the transparent pleura, that its paren- chyma is formed by the aggregation of a multitude of small vesicles of an irregularly spheroid or ovoid figure, full of air, and separated from each other by opaque white partitions. These vesicles, which on the surface of the lungs have the ap- pearance of small transparent points, are not of an uniform size ; the largest are equal to the third or fourth part of a millet-seed. They are grouped in masses or lobules, divided from each other by par- titions of closelv condensed cellular membrane, very thin, yet thicker and more opaque than the partitions between the individual cells. These partitions traverse the pulmonary substance in all directions, and crossing each other under various angles, form figures of different shapes, such as lozenges, squares, trapeziums, or irregular trian- gles, ihe bounding lines of which are rendered still more defined by the black pulmonary matter that is deposited along them. (Forbes's Transla- tion of Laennec.) If we analyze this structure, we find that it is composed, 1st, of the minuter ramifications of the bronchi, which go on subdividing and diminishing in caliber until they terminate each in a cul-de-sac or air-cell, as it is commonly termed, of extreme delicacy and minuteness, on the parietes of which the pulmonary vessels ramify in an extreme state of fineness, (Keisse;srn, De Structural Pulmo- niini;) and 2dly, of the common cellular mem- brane which serves to connect these air-cells together, and which likewise forms several mem- branous partitions that divide each lobe into a number of distinct lobules, and is hence termed the interlobular cellular tissue, each lobule being as perfect I v isolated from those adjoining it by Vol. II 3 u* this partition, as each lobe is by its investiture of pleura. Each of these textures is liable to emphysema, and hence we have two varieties of this disease in the lung: 1. the vesicular or true pulmonary emphysema, (as it is somewhat arbitrarily termed by Laennec.) formed by the dilatation of the minute bronchi and air-cells, or by the rupture of their parietes, by which several contiguous cells are thrown into one; 2. the interlobular emphy* sema, formed by the infiltration of air into the interlobular cellular tissue. The former usually occurs as a chronic disease, while the latter as generally assumes the character of an acute affec- tion. I. PtJLMOXATlY OR VesICULAH EwPHTSEWA. In pulmonary emphysema, the size of the air-cells is much increased and is less uniform. The greater number equal or exceed the size of a millet-seed, while some attain the magnitude of hemp-seed, cherry-stones, or even French beans. (Laennec.) We arc disposed to think, however, that cavities of such a size are rarely formed by the dilatation of individual cells, as in more than one hundred dissections which we have made of pulmonary emphysema, we never except in one instance saw the air-cells dilated to the size of a garden-pea ; in the great majority of cases the cavities of this size, or even of a less diameter, are formed by several ceils being thrown into one, in consequence of their delicate partitions being overstrained and ruptured. In some cases, the walls of Ihe cells disappear from one entire lobule, leaving only some lacerated filaments traversing its cavity from one interlobular partition to another, and in some instances these partitions are also lacerated, and their respective lobules are thus thrown into one large cavity, which usually reaches the surface of the lung, and forms a projection under the pleura. In order to see these alterations of structure, it is necessary to inflate the lung and dry it previous to examination, as without this precaution the cells collapse immediately when cut into, and all appearance of emphysema is consequently lost. Emphysema may affect both lungs at the same time, one only, or a part of one, or both: in the latter case, and, indeed, in any case, as long as the disease is confined to a simple dilata- tion of the cells, or to the rupture of a few of their partitions, and does not form vesicles of any con- siderable size on the surface of the lung, it may be easily overlooked in the dead body ; for this reason, the disease, which is really one of the most constant morbid appearances in all cases of protracted dyspnoea, has been as constantly over- looked, and in this way the lungs of asthmatic patients have been regarded as healthy when they are in reality emphysematous, and cases of dys- pnoea set down as nervous or idiopathic, for which anatomy has now discovered an organic cause. When the disease exists in a very high de- gree, we cannot help being struck with the ap- pearance of the parts. The lungs seem as if 1 confined within their natural cavity, and when I exposed, instead of collapsing as usual, they rise i in some degree, and project beyond the borders ' of the thorax. If we examine them in this state, they feel firmer than natural, and it is more than j usually difficult to flatten them. The crepitation](https://iiif.wellcomecollection.org/image/b21116775_0017.jp2/full/800%2C/0/default.jpg)