Volume 1
The science and art of surgery : a treatise on surgical injuries, diseases, and operations / by John Eric Erichsen.
- John Eric Erichsen
- Date:
- 1895
Licence: Public Domain Mark
Credit: The science and art of surgery : a treatise on surgical injuries, diseases, and operations / by John Eric Erichsen. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
161/1274 (page 129)
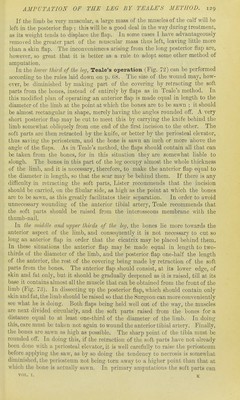
![If the limb be very rausculav, a large mass of the muscles of the calf will be left in the posterior flap ; this will be a good deal in the way during treatment, as its weight tends to displace the flap. In some cases I have advantageously removed the greater part of the n)uscular mass thus left, leaving little more than a skin flap. The inconveniences arising from the long posterior flap are, liowever, so great that it is better as a rule to adopt some other method of amputation. In the lower third of the leg, Teale's operation (Fig. 72) can be performed according to the rules laid down on p. G8. The size of the wound may, how- ever, be diminished by making part of the covering by retracting the soft parts from the bones, instead of entirely by flaps as in Teale'a method. In this modified plan of operating an anterior flap is made equal in length to the diameter of the limb at the point at Avhich the bones are to be sawn ; it should be almost rectangular in shape, merely having the angles rounded off. A very short posterior flap may be cut to meet this by carrying the knife behind the limb somewhat obliquely from one end of the first incision to the other. The soft parts are then retracted by the knife, or better by the periosteal elevator, thus saving the periosteum, and the bone is sawn an inch or more above the angle of the flaps. .As in Teale's method, the flaps should contain all that can be taken from the bones, for in this situation they are somewhat liable to slough. The bones in this part of the leg occupy almost the whole thickness of the limb, and it is necessary, therefore, to make the anterior flap equal to the diameter in length, so that the scar may be behind them. If there is any difficulty in retracting the soft parts, Lister recommends that the incision should be carried, on the fibular side, as high as the point at which the bones are to be sawn, as this greatly facilitates their separation. In order to avoid unnecessary wounding of the anterior tibial artery, Teale recommends that the soft parts should be raised from the interosseous membrane with the thumb-nail. In the viiclclU and tqjjwr thirds of the leg, the bones lie more towards the anterior aspect of the limb, and consequently it is not necessary to cut so long an anterior flap in order that the cicatrix may be placed behind them. In these situations the anterior flap may be made equal in length to two- thirds of the diameter of the limb, and the posterior flap one-half the length of the anterior, the rest of the covering being made by retraction of the soft parts from the bones. The anterior flap should consist, at its lower edge, of skin and fat only, but it should be gradually deepened as it is raised, till at its base it contains almost all the muscle that can be obtained from the front of the limb (Fig. 73). In dissecting up the posterior flap, which should contain only skin and fat, the limb should be raised so that the Surgeon can more conveniently see what he is doing. Both flaps being held well out of the way, the muscles are next divided circularly, and the soft parts raised from the bones for a distance equal to at least one-third of the diameter of the limb. In doing this, care must be taken not again to wound the anterior tibial artery. Finally, the bones are sawn as high as possible. The sharp point of the tibia must be rounded off. In doing this, if the retraction of the soft parts have not already been done with a periosteal elevator, it is well carefully to raise the periosteum before aj)])lyiiig the saw, as by so doing the tendency to necrosis is somewhat diminished, the periosteum not being torn away to a higher point than that at which the bone is actually sawn. In primary amputations the soft parts can VOL. I. K](https://iiif.wellcomecollection.org/image/b21510969_0001_0161.jp2/full/800%2C/0/default.jpg)