Paediatric implications for some adult disorders : Scientific proceedings of the 4th Unigate Workshop, held at the Royal Academy of Physicians, St. Andrews Place, London, N.W. 1, May 1976 / edited by Donald Barltrop.
- Unigate Paediatric Workshop 1976 : Royal College of Physicians)
- Date:
- 1977
Licence: Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0)
Credit: Paediatric implications for some adult disorders : Scientific proceedings of the 4th Unigate Workshop, held at the Royal Academy of Physicians, St. Andrews Place, London, N.W. 1, May 1976 / edited by Donald Barltrop. Source: Wellcome Collection.
20/168 page 8
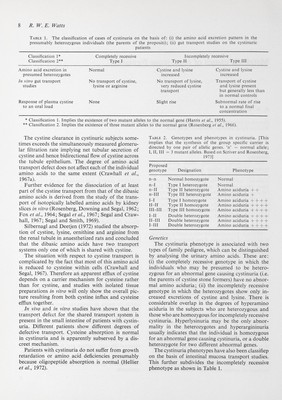
![8 R. W. E. fVatts Table 1. The classification of cases of cystinuria on the basis of: (i) the amino acid excretion pattern in the presumably heterozygous individuals (the parents of the propositi); (ii) gut transport studies on the cystinuric patients Classification 1* Completely recessive Incompletely recessive Classification 2** Type 1 Type II Type III * Classification 1. Implies the existence of two mutant alleles to the normal gene (Harris et al., 1955). ** Classification 2. Implies the existence of three mutant alleles to the normal gene (Rosenberg et al., 1966). The cystine clearance in cystinuric subjects some¬ times exceeds the simultaneously measured glomeru¬ lar filtration rate implying net tubular secretion of cystine and hence bidirectional flow of cystine across the tubule epithelium. The degree of amino acid transport defect does not affect each of the individual amino acids to the same extent (Crawhall et al., 1967a). Further evidence for the dissociation of at least part of the cystine transport from that of the dibasic amino acids is derived from the study of the trans¬ port of isotopically labelled amino acids by kidney slices in vitro (Rosenberg, Downing and Segal, 1962; Fox et al., 1964; Segal et ai, 1967; Segal and Craw¬ hall, 1967; Segal and Smith, 1969). Silbernagl and Deetjen (1972) studied the absorp¬ tion of cystine, lysine, ornithine and arginine from the renal tubule in anaesthetized rats and concluded that the dibasic amino acids have two transport systems only one of which is shared with cystine. The situation with respect to cystine transport is complicated by the fact that most of this amino acid is reduced to cysteine within cells (Crawhall and Segal, 1967). Therefore an apparent efflux of cystine depends on a carrier mechanism for cysteine rather than for cystine, and studies with isolated tissue preparations in vitro will only show the overall pic¬ ture resulting from both cystine influx and cysteine efflux together. In vivo and in vitro studies have shown that the transport defect for the shared transport system is present in the small intestine of patients with cystin¬ uria. Different patients show different degrees of defective transport. Cysteine absorption is normal in cystinuria and is apparently subserved by a dis¬ creet mechanism. Patients with cystinuria do not suffer from growth retardation or amino acid deficiencies presumably because oligopeptide absorption is normal (Hellier et al., 1972). Table 2. Genotypes and phenotypes in cystinuria. [This implies that the synthesis of the group specific carrier is directed by one pair of allelic genes, 'n' = normal allele; I, П, III = 3 mutant alleles. Based on Scriver and Rosenberg, 1973] Proposed genotype Designation n-n n-I n-II n-III I-I II-II iri-m i-ii ii-iii i-iii Phenotype Normal Normal Amino aciduria + + Amino aciduria + Amino aciduria + -b + + Amino aciduria + + + + Amino aciduria + + + + Amino aciduria + + + + Amino aciduria + + + + Amino aciduria + + + + Normal homozygote Type I heterozygote Type II heterozygote Type III heterozygote Type I homozygote Type II homozygote Type III homozygote Double heterozygote Double heterozygote Double heterozygote Genetics The cystinuria phenotype is associated with two types of family pedigree, which can be distinguished by analysing the urinary amino acids. These are: (i) the completely recessive genotype in which the individuals who may be presumed to be hetero¬ zygous for an abnormal gene causing cystinuria (i.e. the parents of cystine stone formers) have no abnor¬ mal amino aciduria; (ii) the incompletely recessive genotype in which the heterozygotes show only in¬ creased excretions of cystine and lysine. There is considerable overlap in the degrees of hyperamino aciduria in the subjects who are heterozygous and those who are homozygous for incompletely recessive cystinuria. Hyperlysinuria may be the only abnor¬ mality in the heterozygotes and hyperargininuria usually indicates that the individual is homozygous for an abnormal gene causing cystinuria, or a double heterozygote for two different abnormal genes. The cystinuria phenotypes have also been classifiep on the basis of intestinal mucosa transport studies. This further subdivides the incompletely recessive phenotype as shown in Table 1.](https://iiif.wellcomecollection.org/image/b18031298_0021.JP2/full/800%2C/0/default.jpg)