Paediatric implications for some adult disorders : Scientific proceedings of the 4th Unigate Workshop, held at the Royal Academy of Physicians, St. Andrews Place, London, N.W. 1, May 1976 / edited by Donald Barltrop.
- Unigate Paediatric Workshop 1976 : Royal College of Physicians)
- Date:
- 1977
Licence: Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0)
Credit: Paediatric implications for some adult disorders : Scientific proceedings of the 4th Unigate Workshop, held at the Royal Academy of Physicians, St. Andrews Place, London, N.W. 1, May 1976 / edited by Donald Barltrop. Source: Wellcome Collection.
24/168 page 12
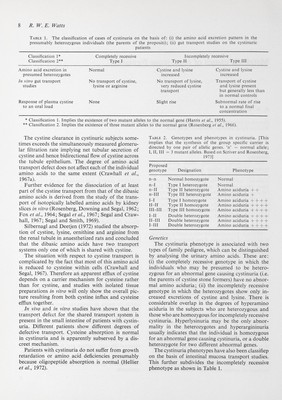
![12 R. W. E. Watts Genetics The data are compatible with both types of pri¬ mary hyperoxaluria being due to the operation of rare autosomal recessive mutant genes. The hetero¬ zygous carriers excrete normal amounts of oxalate and have not so far proved to be detectable on clini¬ cal or biochemical grounds. Pathological features In the early stages, the pathological findings are confined to the kidneys, and comprise variable de¬ grees of hydrocalycosis and hydronephrosis. Inter¬ stitial deposits of calcium oxalate form later causing severe renal fibrosis and shrinkage and imparting a tough gritty feel to the organ when it is incised. The changes of secondary pyelonephritis and renal hypertension sometimes complicate the pathological picture. The renal tubules may be blocked by aggre¬ gated calcium oxalate crystals, and this is especially likely if the terminal illness is precipitated by a hypotensive-oliguric episode. Systemic calcium oxalate deposits (oxalosis) are a striking histopathological feature. The characteristic rosette-like calcium oxalate monohydrate crystals are highly biréfringent and easily recognized in the polarizing microscope. Their full extent will be apparent if the unfixed tissue is examined, but they are sufficiently insoluble for some to remain after routine fixation in aqueous fixatives. They occur most extensively in the myocardium, the tunica media of the muscular arteries and arterioles, the rete testis and at sites of rapid bone turnover. A few crystals can be found in association with the arterial supply of all the organs, and some have been found intra-axonally in peripheral nerves. Clinical features The two biochemically distinct types of primary hyperoxaluria do not appear to be clinically dis¬ tinguishable. Most patients (the juvenile type) present with urolithiasis during the first decade and die before they are twenty years old. The terminal rapidly progressive uraemic illness usually only lasts a few months and appears to be associated with a rapid increase in the amount of calcium oxalate deposited in the kidneys, which are already damaged by fibrosis, calculous disease, and some degree of calcium oxalate nephrocalcinosis and secondary pyelonephritis. The terminal phase of rapidly pro¬ gressing uraemia usually only lasts a few months and appears to be associated with the rapid increase in renal oxalosis and with the development of sys¬ temic oxalosis. Intracardiac conduction defects with bradycardia and complete heart block may develop during the terminal illness. These may be due to the situation of myocardial calcium oxalate deposits, to sequestration of calcium ions or to the presence of local high concentrations of glyoxylate ions. Ischae- mic lesions occur on the extremities especially in the pulps of the fingers and toes, and severe acrocyanosis with peripheral gangrene may be observed. The intra- neuronal calcium oxalate deposits are associated with a progressive peripheral neuropathy. The vascular and neurological manifestations have been encoun¬ tered most often in patients who have been haemo- or peritoneally dialysed in the terminal illness, or in whom an attempt has been made to treat the dis¬ order by renal transplantation. A few cases of primary hyperoxaluria (the infan¬ tile type) follow an unusually rapid course with fits and progressive renal failure in the early months of life. Another group (the adult type) follow a more benign course, presenting in adult life and surviving with intermittent stone formation into the fourth or fifth decade and, more rarely, even later. However, the amount of oxalate excreted and the age at which renal failure develops are only loosely correlated, and it is not known if these clinical types represent biochemically definable variants of the disease. Primary hyperoxaluria can only be diagnosed by chemical measurement of urinary oxalate excretion. Isotope dilution analysis is a valuable reference method or research tool and the two diff'erent methods based on this principle (Hockaday et al, 1965; Gibbs and Watts, 1969) give identical values for the upper limit of the normal range [55 mg anhy¬ drous oxalic acid (0-6 mmol) per 24 hr per 1-73 m^ body surface area]. There are no diagnostically significant difi'erences between the sexes or for child¬ ren when the results are related to the body surface areas. Chemical methods generally give lower values, due to incomplete recovery, especially in the normal range, although they are suitable as a screen for primary hyperoxaluria and are reviewed in detail by Hodgkinson (1970). It is claimed that a recently developed enzyme method (Hallson and Rose, 1974) which is suitable for routine use gives results which agree with those obtained by isotope dilution analysis more closely than chemical methods. Patients with primary hyperoxaluria excrete at least about twice the upper normal level. A few patients with recurrent urinary stones have much smaller increases than this and they should be regarded as having a diff'erent and at present undefined disorder. These smaller in¬ creases in urinary oxalate excretion may be more amenable to dietary manipulation. Urinary oxalate measurements are unreliable in the terminal phases of the illness when apparently normal values may be obtained because of the rapidly developing oxalate deposits in the renal tubules. The urinary glycolate excretion is approximately equimolar with the oxalate excretion in normal sub¬ jects and in patients with Type I primary hyperoxal¬ uria. The glyoxylate excretion is increased about 3](https://iiif.wellcomecollection.org/image/b18031298_0025.JP2/full/800%2C/0/default.jpg)