Physical diagnosis of diseases of the chest / by Richard C. Cabot.
- Richard Clarke Cabot
- Date:
- 1903
Licence: Public Domain Mark
Credit: Physical diagnosis of diseases of the chest / by Richard C. Cabot. Source: Wellcome Collection.
Provider: This material has been provided by the Francis A. Countway Library of Medicine, through the Medical Heritage Library. The original may be consulted at the Francis A. Countway Library of Medicine, Harvard Medical School.
275/346 (page 253)
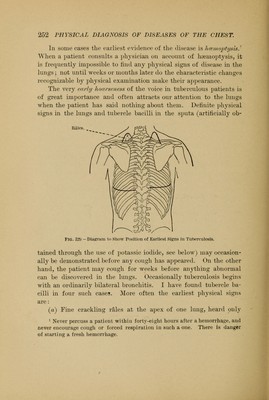
![with or after cough and at the end of inspiration. [More rarely squeaks may be heard.] (See Fig. 129). (b) A slight diminution in the excursion of the diaphragm on the affected side, as shown by Litten's diaphragm shadow. (c') Slight diminution in the intensity of the respiratory mur- mur, with or without interrupted inspiration (''cog-wheel breath- ing). (a) In examining the apices of the lungs for evidence of early tuberculosis one should secure if possible perfect quiet in the room, and have the clothes entirely removed from the patient's chest. The ordinary hard-rubber chest-piece is better than the chest-piece of the Bowles instrument when we wish to search the apices for fine rales. After listening during quiet breathing over the apices above and below the clavicle in front, and above the spine of the scapula behind, the patient should be directed to breathe out and then, at the end of expiration, to cough. During the deep inspiration which is likely to precede or to follow such a cough one should listen as carefully as possible at the apex of the lung, above and below the clavicle, concentrating attention especially upon the last quarter of the inspiration, when rales are most apt to appear. Sometimes only one or two crackles may be heard with each inspi- ration, and not infrequently they Avill not be heard at all unless the patient is made to cough, but even a single vale, if persistent,' is important. In children who cannot cough at will, one can accom- plish nearly the same result by making them count as long as pos- sible with one breath and then listening to the immediately suc- ceeding inspiration. When listening over the apex of the lung, one should never allow the patient to turn his head sharply in the other direction, since such an attitude stretches the skin and mus- cles on the side on which we are listening so as to produce annoy- ing muscle sounds or skin rubs. In cases in which one suspects that incipient tuberculosis is 1 Rales heard only during the first few breaths and not found to persist on subsequent examinations, may be due to the expansion of atelectatic lobules.](https://iiif.wellcomecollection.org/image/b21175871_0275.jp2/full/800%2C/0/default.jpg)