Treatise on the diseases of the eye : including the anatomy of the organ / by Carl Stellwag von Carion ; tr. from the 3rd German ed. and ed. by Charles E. Hackley and D.B. St. John Roosa ; with an appendix by the editors.
- Karl Stellwag von Carion
- Date:
- 1870
Licence: Public Domain Mark
Credit: Treatise on the diseases of the eye : including the anatomy of the organ / by Carl Stellwag von Carion ; tr. from the 3rd German ed. and ed. by Charles E. Hackley and D.B. St. John Roosa ; with an appendix by the editors. Source: Wellcome Collection.
Provider: This material has been provided by the Francis A. Countway Library of Medicine, through the Medical Heritage Library. The original may be consulted at the Francis A. Countway Library of Medicine, Harvard Medical School.
737/810 page 715
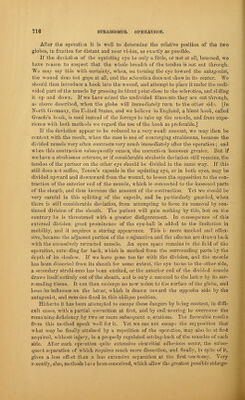
![nent. If an operation be performed very early, in periodical strabismus—the cor- rection of those conditions which cause the innervation to be directed to deviation, being often very difficult or impossible—nothing is gained. The same difficulties continue to exist after the operation, and if the causes be not removed the strabis- mus is very apt to return. But if the strabismus has become fixed, it is still less justifiable, to anticipate the possibility of outgrowing the strabismus, since with- out it there is scarcely any hope of a restoration of binocular vision. On the con- trary, too long a postponement of the operation is not to be advised, because the organic changes of the affected muscle may become troublesome with the lapse of time, and necessitate an increase in the amount of setting-back, and with this increase the disadvantages and dangers of the operation. Where the strabismus is developed later in life, or especially where absolute or rela- tive insufficiency of a muscle is the proximate cause, there scarcely remains any great space of time in which to choose the operation. Tenotomy is best done as soon as the other means have proved insufficient. But here also the result frequently is not up to the expectations, even when the fundamental disease is not progressive, and a correc- tion which at the time of operation was sufficient, afterward proves to be not enough. 6. The operation requires no preparation, and is generally undertaken on patients who are going about as usual. The instruments required for the performance of the operation are a medium- sized forceps, a pair of small scissors, curved on the flat, and some small sponges [or bits of fine, soft muslin] to take up the blood. It is of advantage to undertake the operation while the patient is under the influence of an anaesthetic. The muscles then become relaxed, and are more easily lifted from the globe and divided. The patient should be on his back, and in case an anaesthetic be not used, the other eye should be closed by a blindage, in order that the patient may have more power over the one to be operated upon, and be able to turn it as may be required. The assistant should open the lids as widely as possible, and hold them, while at the same time he prevents any movements of the head. Another assistant removes the blond. The eye is now turned toward the antago- nist of the squinting muscle, or held there by the fixation forceps, while the surgeon seizes the conjunctiva directly over the line of insertion of the tendon to be divided, three lines from the corneal border, lifts up a fold, and cuts through it vertically with the scissors. Then the wound is enlarged above and below to the dis- tance of about four lines. When this has been done, the forceps are placed in the wound perpendicular to the surface of the globe, and its points hugging the sclero- tica are pushed a little backward, so that the muscle comes between the branches, and after the closure of the forceps, it maybe drawn in an acute angle out of the wound. At the same time the scissors are placed in the wound with the other hand, one blade placed under the muscle (see fig. 93), and the tendon divided close to the sclerotica.](https://iiif.wellcomecollection.org/image/b2107902x_0737.jp2/full/800%2C/0/default.jpg)