Discussion on the diagnosis and treatment of abcess of the brain : opening papers.
- Date:
- [1934?]
Licence: In copyright
Credit: Discussion on the diagnosis and treatment of abcess of the brain : opening papers. Source: Wellcome Collection.
10/44 (page 1652)
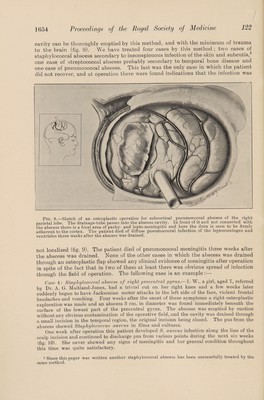
![collected. At the second dressing on April 25 a considerable amount of pus was found in the dressings, and there was a little more at the next dressing on April 30. On May 3 the tube was removed and replaced by a strip of folded gutta-percha and this was removed on May 7. The patient made a complete recovery. Skiagrams, taken while the catheter was still in the brain (fig. 8), show that it had been passed in a somewhat medial direction and this probably explains why it did not enter the abscess cavity at the time of operation. This patient had fairly severe rise of intracranial pressure before operation, but she was not drowsy or lethargic and consequently there was no need for immediate evacuation of the abscess. If the patient’s condition is so urgent that immediate drainage of the abscess is necessary, and the rubber catheter will not go in, it is best to use a firm intratracheal catheter and even to put a stilette in its interior while it is being passed. If the abscess is very deep-seated (i,e. 4 to 5 cm. or more) and the catheter cannot be pushed into it, it is usually best to leave the brain needle in situ, or, as recommended by Coleman, to mount a cannula on the brain needle and when the abscess has been entered to withdraw the needle leaving the cannula in place. A brain needle with an adjustable flange has been designed by one of us [C. D.] for cases of this type. Sometimes the pus encountered may be too thick to pass through a brain needle. In such cases drainage by the closed method will be ineffective and the abscess must be emptied by suction under direct vision. Drainage by Open Methods Drainage by open methods may be done through a limited opening in the skull over the abscess, or by wide osteoplastic exploration. (a) Through a limited openingFor drainage by direct vision it is usually necessary to have an opening in the skull and dura 3 to 4 cm. in diameter. After the pus is found with a needle, the cortex is incised and some special form of retractor such as a bivalve speculum is passed down into the abscess. Adherents of this method lay stress on the importance of passing the drain down to the depths of the abscess cavity (McKenzie [5]). Various forms of drainage are employed ; a large drainage tube, gauze packing, cone-shaped wire-mesh drain and so forth. We believe that this form of operation is satisfactory when the abscess is super¬ ficial, but there are serious objections to it in deep-seated abscesses. Everyone who has tried to use this method for deep-seated abscesses will have experienced the great difficulty in getting exposure of the abscess through such a small opening. The oedematous brain overlying the abscess pushes itself into the wound, no matter what form of retraction is used, and rapidly obscures the abscess, which may not be found again. In operations of this type opportunity of inspecting the abscess may be very fleeting and everything has to be done so rapidly (the evacuation of the pus, and insertion of the drainage tube to the bottom of the abscess cavity), that there is no room for the slightest hitch. Just at the moment of exposure of the abscess the depths of the field may be hidden by fresh bleeding from cortical vessels, which have been ruptured by the deeper and stronger retraction that is necessarily though unconsciously made when the abscess is exposed. The method is too hazardous for deep-seated abscesses, though it is probably the method of choice for superficial ones. With this method also it is possible to irrigate the abscess cavity, a procedure employed by Macewen [6] in his conspicuously successful group of cases. {h) Through an osteoplastic flap.—Neurological surgeons occasionally come upon a brain abscess when exploring for intracranial tumour by the usual wide osteo¬ plastic exploration. In such cases the abscess is generally a chronic one of fairly long duration and perhaps for that reason these cases often make complete recovery. Nevertheless, one cannot help being impressed with the ease with which an abscess](https://iiif.wellcomecollection.org/image/b3062986x_0010.jp2/full/800%2C/0/default.jpg)