The American text-book of operative dentistry / In contributions of eminent authorities. Ed. by Edward C. Kirk.
- Edward Cameron Kirk
- Date:
- 1900
Licence: Public Domain Mark
Credit: The American text-book of operative dentistry / In contributions of eminent authorities. Ed. by Edward C. Kirk. Source: Wellcome Collection.
Provider: This material has been provided by the Augustus C. Long Health Sciences Library at Columbia University and Columbia University Libraries/Information Services, through the Medical Heritage Library. The original may be consulted at the the Augustus C. Long Health Sciences Library at Columbia University and Columbia University.
790/864 (page 788)
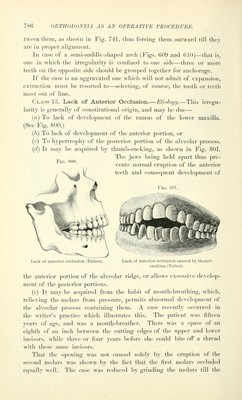
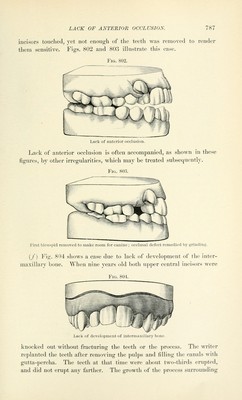
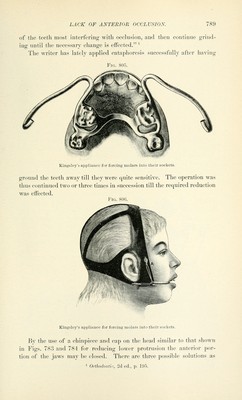
![these teeth was jirrcstcd and lliat ol' the iiitcnnaxillai'y bone and ad- jacent part of the uj)i)('r maxilla retarded as shown. The cast was made at the age of sixteen, at which time one of the teeth was still so firm as to permit the insertion of a gold filling, while the other was so loose from resorption of the root that it was extracted. The socket was deepened and enlarged and a tooth implanted. The infincnce of heredity may he prominent in this deformity, several meml)ers of one family presenting the condition. AMiile this irregularity is generally of constitutional origin it is not always dtjveloped till the eruption of the second and tliii-d molars, or, if slight, while the first molar is the posterior tooth, is increased in de- gree by the eruption of the second and the third molars, just as a pair of dividers kept open a certain distance by a prop two inches from the joint will be opened farther if a prop of the same height be placed between the first one and the joint. The writer has been fortunate enough to be able to watch the devel- opment, in its later stages, of such a case. The occlusion at the first visit of the patient was entirely with the second molars, and the cut- ting edges of the upper and lower incisors were a quarter of an inch apart. As the patient had suffered during childhood from what she called bone disease she was afraid to submit to any treatment for bringing the anterior portion of the jaws nearer together. Gold crowns were placed over the lower first molars, to occlude with upper teeth, and increase the power of mastication. Within two or three years afterward the third molars erupted and opened the jaws to such an extent that the gold crowns lacked more than a sixteenth of an inch of touching the upper teeth. This case was undoubtedly due to the shortness of the ramus of the lower jaw. Treatment.—The simplest treatment of such cases is to grind down the cusps of the occluding teeth. In simple cases this can be done so as to enable the incisors to bite upon each other. (See Figs. 802 and 80.3.) The third molars may interfere so much that their extraction will be indicated. By the use of articulating paper the occluding points whi(;h need grinding may be easily located. In some cases there may be a mal-occlusion of the cusps only, so that grinding them away will be sufficient, while in other cases a con- siderable portion of the tooth must be ground away. Prof. Guilford suggests grinding as much as possible without causing too great pain, and then administering an anesthetic and continuing the grinding. The sensitiveness of the exposed dentin may afterward be obtunded by repeated applications of either zinc chlorid, caustic potash [potas- sium hydroxid], or silver nitrate. Where neither of these will avail sufficiently, it may be advisable to devitalize the pulps of two or more](https://iiif.wellcomecollection.org/image/b21216629_0790.jp2/full/800%2C/0/default.jpg)