Volume 1
A manual of operative surgery / by Sir Frederick Treves.
- Sir Frederick Treves, 1st Baronet
- Date:
- 1903
Licence: Attribution-NonCommercial 4.0 International (CC BY-NC 4.0)
Credit: A manual of operative surgery / by Sir Frederick Treves. Source: Wellcome Collection.
Provider: This material has been provided by The University of Leeds Library. The original may be consulted at The University of Leeds Library.
720/808 (page 700)
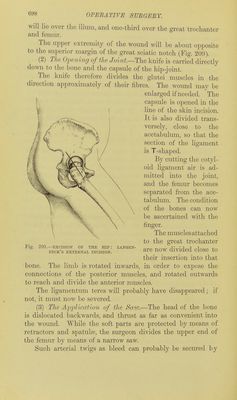
![have been urged against the retention of the trochanter, and advises that under any circumstances as Httle bone should be taken away as possible, compatibly with thorough removal of the diseased portions. This operation follows very emphatically the lines of the open method, and is a little crude and a little regardless of the tissues in the vicinity of the joint. It may claim to be easy and safe. The bone is well and readily exposed, and is very easily sawn. Good drainage is allowed for. The disadvantages of the method are the following :—Many large and important muscles arc cut through, and the stability of the new joint possibly weakened thereby. The soft parts are exposed to much handling and some bruising. Many of the arteries which meet about the great trochanter are divided. A transverse section is made of the capsule, and the strength of that ligament is consequently weakened. 2. By the Subperiosteal Method. (1) T/te Incision, and the Exposure of tJte Neck of tJte Femur.—The incision is precisely similar to that just described; and the positions of the patient, of the limb, and of the surgeon, are identical with those observed in the previous operation. The skin and subcutaneous fat are divided, and the part of the gluteus maximus muscle which is exposed is severed in the line of the skin incision, and the gap thus made in the muscles is widened by means of suitable retractors (Fig. 210). The surgeon now seeks with the linger for the gap between the gluteus medius (in front and above) and the pyriformis (behind and below). These two muscles are separated from one another,, and in the gap between them and in the line of the original -incision the knife is carried down to the great trochanter, the periosteum of which is divided (Fig. 2]0). Now with one broad retractor the gluteus medius is dra^vn forwards and the pyriformis backwards, and the capsule, which is thereby exposed, is divided with the knife in the long axis of the femoral neck. Passing through the capsule, the surgeon divides the periosteum of the neck in the same line, and continues this periosteal incision downwards over the upper margin of the](https://iiif.wellcomecollection.org/image/b21511342_0001_0722.jp2/full/800%2C/0/default.jpg)