The mechanism of dislocations and fracture of the hip . Litholapaxy, or, Rapid lithotrity with evacuation / by Henry Jacob Bigelow.
- Henry Jacob Bigelow
- Date:
- 1900
Licence: Public Domain Mark
Credit: The mechanism of dislocations and fracture of the hip . Litholapaxy, or, Rapid lithotrity with evacuation / by Henry Jacob Bigelow. Source: Wellcome Collection.
75/372 (page 63)
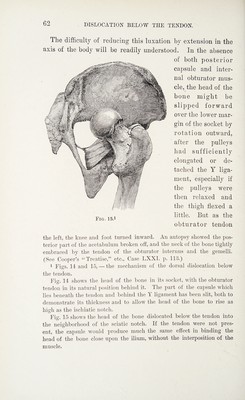
![and its subjacent capsule now lie between the head of the bone and the socket, they oppose the entrance of the head by a firm tendinous wall, which is drawn down as the head descends, and which no extension or rotation, short of its rupture, can displace or overcome. The muscle is tense, and in its turn renders the ligament more tense, carrying the head of the bone backward and upward toward the ischiatic notch. The inversion, flexion, and adduction of the limb are thus augmented by the com¬ bined and reciprocal action of the ligament and the obturator muscle, — the latter being aided by the subjacent capsule, when that remains untorn.1 1 It has been before said that if the neck of the femur be farther driven upward so as to rupture the obturator tendon and capsule, the luxation will become simply dorsal. Malgaigne correctly says that “the ischiatic luxation leads frequently to the iliac luxation ; ” but he fails to identify the mechanism of the change when he asks, “ May not the for¬ mer also be consecutive to the latter, in view of the fact that by flexion or strong traction the head of the bone may be drawn downward from the dorsum to the notch ? ” (“ Traite,” etc., p. 831.) In the high dorsal dislo¬ cation the small rotators would be so lacerated by the ascent of the bone or by drawing it down to reduce it, when engaged in their interstices, that the luxation “ on the ischiatic notch ” would lose its distinctive fea¬ tures. In an interesting discussion upon a pathological specimen of hip luxation of five months’ standing, where an unsuccessful attempt had been made to reduce the bone by longitudinal traction, M. Tillaux main¬ tained that “ in backward luxation of the hip the capsule, and not the muscles [notably the obturator], limits the movement of the head of the femur.” (Societe Imperiale de Chirurgie, ler Juillet, 1868. L’Union Medicale, No. /9, p. 5<.) It is true (see pp. 2, 63) that the obturator tendon and the posterior part of the capsule, which is next in strength to the Y ligament, mutually reinforce each other, so that when the head of the bone rises behind the socket it is generally engaged behind both these fibrous walls. But their mechanical action being identical, it is unneces¬ sary to decide which under these circumstances would first be ruptured. The capsule yields fibre by fibre to the ascending bone, while the com¬ parative elasticity of the tendinous muscle preserves it (Fig. 15), until at the moment of the final rupture of the tendon the dislocation has become practically iliac, and can now be reduced, though disadvantage-](https://iiif.wellcomecollection.org/image/b31351670_0075.jp2/full/800%2C/0/default.jpg)