Diseases of the nose and throat, comprising affections of the trachea and oesophagus / by Sir St. Clair Thomson.
- Thomson, St. Clair, 1859-1943
- Date:
- 1912
Licence: In copyright
Credit: Diseases of the nose and throat, comprising affections of the trachea and oesophagus / by Sir St. Clair Thomson. Source: Wellcome Collection.
Provider: This material has been provided by Royal College of Physicians, London. The original may be consulted at Royal College of Physicians, London.
113/866 page 89
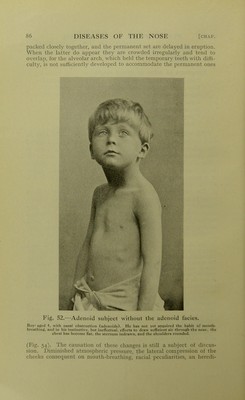
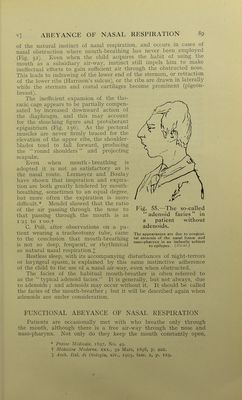
![of the natural instinct of nasal respiration, and occurs in cases of nasal obstruction where mouth-breathing has never been employed (Fig. 52). Even when the child acquires the habit of using the mouth as a subsidiary air-way, instinct still impels him to make ineffectual efforts to gain sufficient air through the obstructed nose. This leads to indrawing of the lower end of the sternum, or retraction of the lower ribs (Harrison's sulcus), or the ribs are drawn in laterally while the sternum and costal cartilages become prominent (pigeon- breast). The inefficient expansion of the tho- racic cage appears to be partially compen- sated by increased downward action of the diaphragm, and this may account for the slouching figure. and protuberant epigastrium (Fig. 156). As the pectoral muscles are never firmly braced for the elevation of the upper ribs, the shoulder- blades tend to fall forward, producing the round shoulders and projecting scapulas. Even when mouth - breathing is adopted it is not as satisfactory as is the nasal route. Lermoyez and Boulay have shown that inspiration and expira- tion are both greatly hindered by mouth- breathing, sometimes to an equal degree, but more often the expiration is more difficult.* Mendel showed that the ratio of the air passing through the nose to Fig. 55.—The so-called that passing through the mouth is as adenoid facias in 1-25 to l oo.t a patient without C. PoH, after observations on a pa- adenoids. tient wearing a tracheotomy tube, came The appearances are due to congeni- tO the conclusion that mouth-breathing tal stenosis of the nasal fossae and , , , 1 n • 1 naso-pharynx in an imbecile subiect IS not so deep, frequent, or rhythmical to epilepsy. {.Kscat.) as natural nasal respiration.;]; Restless sleep, with its accompanying disturbances of night-terrors or laryngeal spasm, is explained by this same instinctive adherence of the child to the use of a nasal air-way, even when obstructed. The facies of the habitual mouth-breather is often referred to as the typical adenoid facies. It is generally, but not always, due to adenoids ; and adenoids may occur without it. It should be called the facies of the mouth-breather ; but it will be described again when adenoids are under consideration. FUNCTIONAL ABEYANCE OF NASAL RESPIRATION Patients are occasionally met with who breathe only through the mouth, although there is a free air-way through the nose and naso-pharynx. Not only do they keep the mouth constantly open, * Presse Mt'dicale, 1897, No. 49. t Mddecine Moderne, xxx., 30 Mars, 1898, p. 201. X Arch. Ital. di Otologia, xiv., 1903, fasc. 2, p. 129.](https://iiif.wellcomecollection.org/image/b23984478_0113.jp2/full/800%2C/0/default.jpg)