Diseases of the nose and throat, comprising affections of the trachea and oesophagus / by Sir St. Clair Thomson.
- Thomson, St. Clair, 1859-1943
- Date:
- 1912
Licence: In copyright
Credit: Diseases of the nose and throat, comprising affections of the trachea and oesophagus / by Sir St. Clair Thomson. Source: Wellcome Collection.
Provider: This material has been provided by Royal College of Physicians, London. The original may be consulted at Royal College of Physicians, London.
135/866 page 111
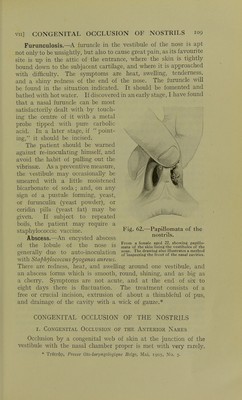
![OBSTRUCTION OF THE GHOAN^ I ] I 3. Congenital Occlusion of the Posterior Cuoan^ This is a comparatively rare condition, due to defect in de- velopment. Pathology.—The obstruction is situated at the posterior choanze, and is found to consist of bone, or partly of membrane and partly of bone. The bony diaphragm is the more common. It may be unilateral or bilateral. It may be complete, or a small opening may exist in it. It is a vestigial structure, being the persistence of the bucco-nasal membrane. Symptoms.—Mouth-breathing and inability to clear the nostril are the chief com- plaints. There is loss of smell in the obstructed nos- tril, and if both are occluded the hearing may be interfered with. In one of my cases the mother had noticed that she could only nurse the child when it was lying on the obstructed side (so that the patent nostril did not get blocked by gravity). There is sometimes a little asym- metry of the face in bilateral occlusion, but there is not the marked atrophy and arch- ing of the palate said to occur when one nostril IS The condition is represented as viewed in the post- .•r • Ti 1 J 1 • nasal mirror. Note the dimpling near the centre artificially occluded m young of the occluding diaphragm, animals. Examination.—The impervious nostril is seen to be filled with a thick, tenacious mucus, which the patient is unable to blow out, and is generally compelled to remove by syringing. The cavity is more spacious than usual, due to the ill-developed con- dition of the turbinals. The mucosa is pale, sodden, and inelastic. If the obstruction is visible from the front it is seen to be pale and grey. In the postnasal mirror it may appear pinkish, and is often dimpled at one point (Fig. 63). A probe will reveal the exact situation and completeness of the partition. Treatment.—The diaphragm must be well broken through, otherwise it is apt to re-form. But this will not take place if the patient is placed under a general anjesthetic, and, with the left forefinger as a guide in the postnasal space, the surgeon breaks it Fig. 63.—Congenital occlusion of the left posterior choana.](https://iiif.wellcomecollection.org/image/b23984478_0135.jp2/full/800%2C/0/default.jpg)