Diseases of the nose and throat, comprising affections of the trachea and oesophagus / by Sir St. Clair Thomson.
- Thomson, St. Clair, 1859-1943
- Date:
- 1912
Licence: In copyright
Credit: Diseases of the nose and throat, comprising affections of the trachea and oesophagus / by Sir St. Clair Thomson. Source: Wellcome Collection.
Provider: This material has been provided by Royal College of Physicians, London. The original may be consulted at Royal College of Physicians, London.
790/866 page 720
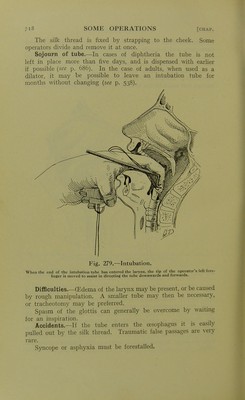
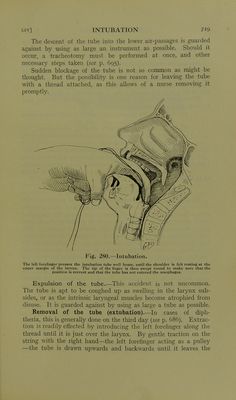
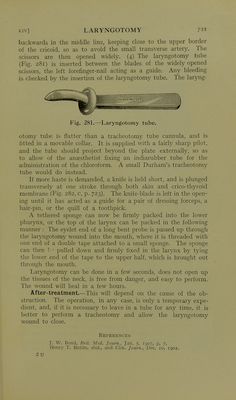
![larynx, and then forwards. If there is no string, the extractor is used on the same hnes as those indicated for effecting the intubation. Enucleation of the tube is in favour in France, The child's head is extended so as to render the larynx prominent. By applying the thumb and forefinger of the right hand on each side and below the cricoid ring, and then pressing upwards, the intubation tube can be shot into the mouth like a stone from a plum. After-treatment.—The patient should not be left for half an hour after extraction, in case of— (a) (Edema of the larynx, which might require introduction of a smaller tube. {])) Spasm of the glottis, with, possibly, convulsions. (c) Paralysis of the dilator (abductor) muscles of the larynx. (d) Subglottic false membrane. All these events would require the reintroduction of the tube. During the operation, as well as in the early after-treatment, a tracheotomy outfit should always be at hand in case of emergencies. Other details, so far as diphtheria is concerned, \vill be 'found at p. 685. LARYNGOTOMY A temporary opening'through the crico-thyroid membrane (Fig. 282, c, p. 723) is indicated (i) in emergencies of sudden laryn- geal stenosis, (2) when the necessary instruments for an urgent tracheotomy are not at hand, or (3) as a prehminary and tem- porary measure in operations on the upper air-passages. This last indication is with the object of {a) making such operations less dangerous; (b) facilitating operation, by suspending the respiration through the mouth and so avoiding coughing and constant sponging; (c) allo\\dng regular administration of the anaesthetic; or (d) avoiding a prehminary tracheotomy. Thus laryngotomy may help to mate operations in the throat and nose more easy, rapid, and efficient. In other circumstances a trache- otomy is preferable. The operation is unsuitable for children, owing to the small size of the larynx (cf. Fig. 206, p. 446). Laryngotomy is thus described by J. W. Bond : The patient's head is extended and held straight in the middle line, (i) An assistant pinches up a vertical fold of skin, so that the centre of it is at the level of the upper border of the cricoid cartilage when the head is extended. (2) The centre of this uphfted fold is then transfixed and cut through so as to make a transverse cut i inch in length. (3) A pair of sharp-pointed scissors, curved on the flat, is plunged through the crico-thyroid membrane downwards and](https://iiif.wellcomecollection.org/image/b23984478_0794.jp2/full/800%2C/0/default.jpg)