Cases of aneurism of the aorta, treated by the iodide of potassium / by Byrom Bramwell.
- Byrom Bramwell
- Date:
- 1878
Licence: Public Domain Mark
Credit: Cases of aneurism of the aorta, treated by the iodide of potassium / by Byrom Bramwell. Source: Wellcome Collection.
Provider: This material has been provided by The Royal College of Surgeons of England. The original may be consulted at The Royal College of Surgeons of England.
33/50
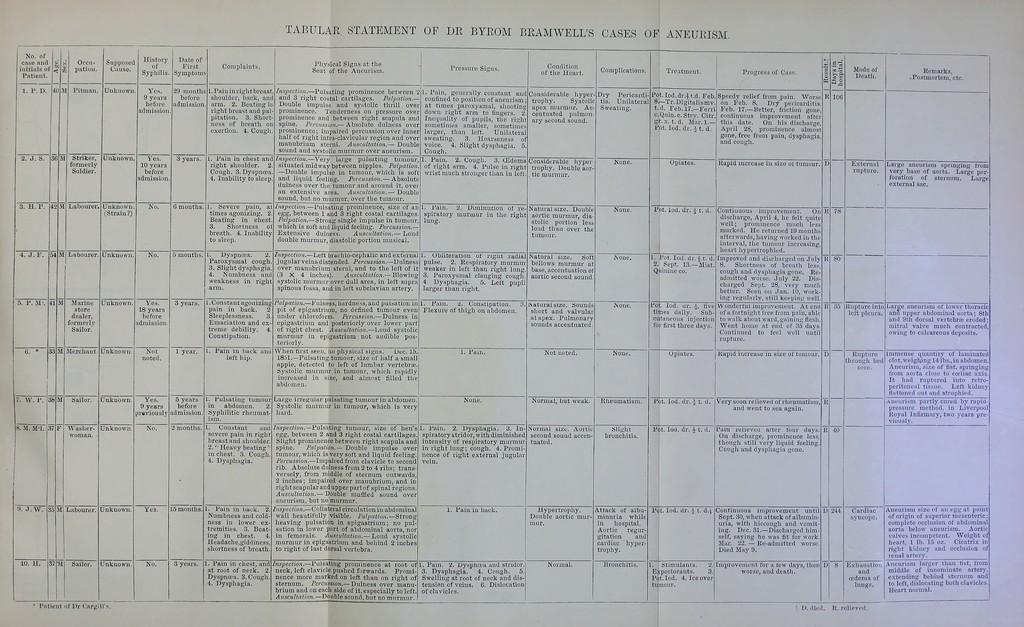
![TABULAE STATEMENT OF DE BYEOM BEAMWELL'S CASES OF ANEUEISM. No. of case and initials of Patient 1. P. D. 2. J. S. 3. H. F. 36 8. M. M'L, 9. J. W. 10. 11. 35 Occu- pation. Supposed Cause. Pitnian. Striker, formerly Soldier. Unknown. Unknown, (Strain ?) 54 M Labourer. Unkno wn. Marine store dealer, formerly Sailor. Merchant Sailor. Was lie r- woman. Labourer, Sailor. History of Syphilis. Vos. 9 year before admission, Yes. 10 years befoi-e admission Date of First Symptom: 29 montlis before admission 3 years. 6 mouths, Yes. 18 years before admission Unkn Unknown. Unknown Unknown. Unknown. Not noted. Yes. 9 years previously No. Yes. Complaints. Physical Signs at the Seat of the Aneurism. l.Pain in right breast, shoulder, back, and arm. 2. BeatiU;^ right breast and pal pitation. 3. Short- ness of breath o exertion. 4. Cougl: Taiu in chest and right slioulder. 2, Cough. 3. Dyspnoea. 4. Inability to sleep. 1. Severe pain, times agonizing. 2 Beating in chest 3. Shortness ol, breath. 4, Inability to sleep. 3 years. 1 year. 5 years before admission. 2 months. 3 years. Dyspnoea, 2. Paroxysmal cough 3. Slight dysphagia. 4. Numbness and weakness in right arm. 1. Constant agonizing pain in back. 2 Sleeplessness. 3. Emaciation and ex- treme debility. Constipation. L. Fain in back ana left hip. 1. Fulsating tumour in abdomen. Syphilitic rheumat- ism . L. Constant iiud severe pain in right breast and shoulder 2. Heavy beating' in cliest. 3. Cough 4. Dysphagia. 1. Fain in back. 2. Numbness and cold- ness in lower ex- tremities. 3. Beat- ing in chest. 4. Headache,giddiness, shortness of breath. Inspection.—Pulsating prominence between 2 and 3 right costal cartilages. Palpation. Double impulse and systolic thrill over prominence. Tenderness on pressure over prominence and between right scapula and spine. Percussion.— Absolute dulness over prominence; impaired percussion over inner half of riglit intra-clavicular region and over manubrium sterni. Auscultation.— Double sound and systolic murmur over aneurism Inspection.—Very large pulsating tumour, situated midway between nipples. Palpation —Double impulse in tumour, -which is soft and liquid feeling. Percussion.— Absolute dulness over the tumour and around it, ovei- an extensive area. Auscultation.— Doubli sound, but no murmur, over the tumour. Inspectiojt.—l-*ulsating prominence, size of an egg, between 1 and 3 riglit costal cartilages, Palpatio7i.~StYoiig single impulse in tumour, which is soft and liquid feeling. Percussion. Extensive dulness. Auscultation.— Loud double murmur, diastolic portion musical Inspection.—Left brachio-cephalic and external jugular veins distended. Percussion.—Dulness over manubrium sterni, and to the left of it (3X4 inches). Aicscultation,— Blowing systolic murmur over dull area, in lelt supra spinous fossa, and in left subclavian artery. Palpation.—Fulness, hardness, and pulsation in pit of epigastrium, no defined tumour even, under chloroform. Percussion.— Dulness in epigastrium and posteriorly over lower part of right chest. Auscultation.—Loud systolic murmur in epigastrium not audible pos- teriorly. Pressure Signs. 1. Pain, generally constant and contined to position of aneurism ; at times paroxysmal, shooting^ down right arm to fingers. 2. Inequality of pupils, the right sometiuu^s smaller, sometimes larger, than left. Unilateral sweating. 3. Hoarseness of voice. 4. Slight dysphagia. 5 Cough. 1. Fain. 2. Cough. 3. U5dema of right arm. 4. Pulse in right Avrist much stronger than in left. Condition of the Heart. Considerable hyper trophy. Systolic apex murmur. Ac- centuated pulmon- ary second sound. Considerable hyper trophy. Double aor- tic murmur. 1. Fain, 2. Diminution of spiratory murmur in the right lung. 1. Obliteration of riglit radial pulse. 2. Respiratory murmur weaker in left than right lung 3. Paroxysmal clanging cough Dysphagia. 5. larger than right. Lett pupil . Pain. 2. Constipation. Flexure of thigh on abdomen. When first seen, no physical signs. Dec. 15,, 1851.—Pulsating tumour, size of half a smallj apple, detucted to left of lumbar vertebrre. Systolic murmur in tumour, which rapidly increased in size, and almost filled the abdomen. Large irregular pulsating tumour in abdomen. Systolic murmur in tumour, which is very hard. Inspection.—Pulsating tumour, size of hen's egg, between 2 and 3 right costal cartilages. Slight prominence between right scapula and spine. Palpation.— Double impulse over tumour, which is very soft and liquid feeling. Percussion.—Impaired from clavicle to second rib. Absolute dulness from 2 to 4 ribs; trans- versely, from middle of sternum outwards, 2 inches; impaired over manubrium, and in rightscapularandupperpartof spinal regions. Auscultation.— Double mufded sound over aneurism, but no murmur. /?is/)eci(on.—Collateral circulation in abdominal wall beautifully visible. Palpation.—Strong heaving pulsation in epigastrium; no pul- sation in lower part of abdominal aorta, nor in femorals. Auscultation.— Loud systolic murmur in epigastrium and behind 2 inches to right of last dorsal vertebra. 1. Pain in chest, and at root of neck. 2. Dyspncea. 3. Cough, 4. Dysphagia. Inspection.—Pulsating prominence at root of neck, left clavicle pushed forwards. Promi- nence more marked on left than on right of sternum. Percussion.— Dulness over manu- brium and on each side of it, especially to left. A7tscuUation.—T)nnh]e sound, but no murmur. None. 1. Pain. 2. Dysphagia. 3. In- spiratory stridor, with diminished intensity of respiratory murmur in right lung; cough. 4. Promi- nence of right external jugular vein. 1. Pain in back. 1. Pain. 2. Dyspntea and stridor. 3. Dysphagia. 4. Cough. 5. Swelling at root of neck and dis- tension of veins. 6. Dislocation of clavicles. Natural size. Double aortic, murmur, dia stolic portion less loud than over the tumour. Natural size. Soft bellows murmur at base, accentuation ol aortic second sound. Complications. Dry Pericardi tis. Unilateral Sweating, None, iNatural size. Sound short and valvular at apex. Pulmonary sounds accentuated Not noted. Normal, but weak- Normal sizt:. Aortic second sound accen- tuated. Hypertrophy. Double aortic mur- mur. Treatment. Progress of Case Pot.Iod.dr.it.d. Feb. 8.—Tr.Digitalismv. t.d. Feb.17.—Ferr c.Quin.c. Stry. Citr gr.x. t. d. Mar.l.- Pot. lod. dr. A t. d. Opiates. Pot. lod. dr. i t. d. I. Pot. lod. dr. ^t. d 2. Sept. 13.—Mist Quinine co. None. Rheumatism. Slight bronchitis. Attack of albu- minuria while in hospital. Aortic regur- gitation and cardiac hyper- trophy. Bronchitis. Pot. lod. or. ^, five times daily. Sub- cutaneous injection for first three days. Opiates. Speedy relief from pain. Worsii on Feb. 8. Dry pericarditis, Feb. 17.—Better, friction gone, continuous improvement after this date. On his discliai April 28, prominence almost gone, free from pain, dysphagia and cough. Rapid increase in size or tumour, Contiuuous improvemenc. On discharge, April 4, he felt quite well; prominence much less marked. Hi; returned 19 mouths afterwards, having worked in the interval, the tumour increasing, heart hypertrophied. Improved and discharged on July 8. Shortness of breath less, cough and dysphagia gone. Re- admitted worse. July 22. D,' charged Sept. 28, very much better. Seen on Jan. 10, work- ing regulnrly, still keeping well Wonderful improvement. At end of a fortnight free from pain, able to walk about ward, gaining flesh. Went home at end of 35 days. Continued to feel well until rupture. Rapid increase in size of tumour. Pot. lod. dr. Very soon relieved of rheumatism and went to sea again. Fbt. lod. dr. A t. d. Pot. lod. dr. ^ t. d.i 1. I Stimulants. 2. Expectorants. 3. Pot. lod. 4. Ice over tumour. Patient of Dr Cargill's. Fain relieveu after four days. On discharge, prominence less, though still very liquid feeling. Cough and dysphagia gone. Continuous improvement until Sept. 30, when attack of albumin- uria, with hiccough and vomit- ing. Dec. 31.—Discharged him- self, saying he was fit for work. Mar. 22. — Re-admitted worse. Died May 9. Improvement for a few days, then worse, and death. 80 Mode of Death. External rupture. Rupture into left pleura Rupture through bed sore. Cardiac syncope. Exhaustion and cedema of lungs. Remarks, .Postmortem, etc. Large aneurism springing trom very base of aorta. Large per- foration of sternum. Large external sac. Large aneurism of lower thoracic ana upper abdominal aorta; 8th and 9th dorsal vertebrae eroded; mitral valve much contracted, owing to calcareous deposits. Immense quantity of lamiuated clot, weighing 14 lbs., in abdomen. Aneurism, size of fist, springing from aorta close to coeliac axis. It had ruptured into retro- peritoneal tissue. Left kidney flattened out and atrophifd. Aneuri.sm partly cured by rapid- pressure method, in Liverpool Royal Infirmary, two years pre- viouslv. Aneurism size of an egg at point of origin of superior mesenteric; complete occlusion of abdominal aorta below aneurism. Aortic valves incompetent. Weight of heart, 1 lb. 15 oz. Cicatrix in right kidney and occlusion of renal artery. Aneurism larger than fist, from middle of innominate artery, extending behind sternum and to left, dislocating both clavicles Heart normal. D, died. R. relieved.](https://iiif.wellcomecollection.org/image/b22279428_0037.jp2/full/800%2C/0/default.jpg)